

High dose versus conventional dose in external beam radiotherapy of prostate cancer: a meta-analysis of long-term follow-up
- PMID: 25173623
- PMCID: PMC11823946
- DOI: 10.1007/s00432-014-1813-1
High dose versus conventional dose in external beam radiotherapy of prostate cancer: a meta-analysis of long-term follow-up
Abstract
Purpose: To assess the efficacy and toxicity between high-dose radiotherapy (HDRT) and conventional-dose radiotherapy (CDRT) by collecting randomized controlled trials of long-term follow-ups.
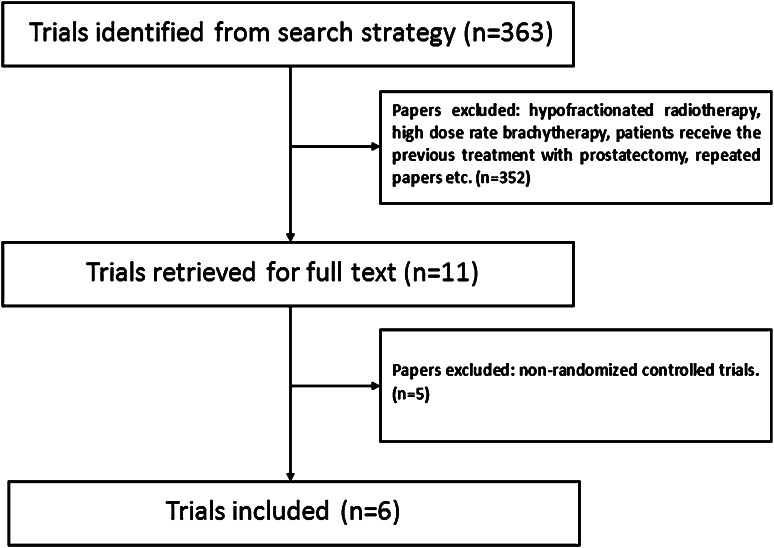
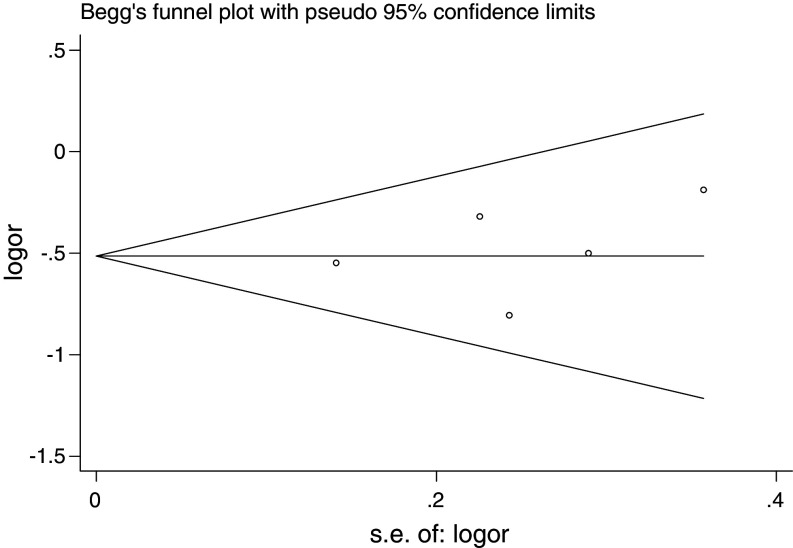
Methods: Unrestricted by language, we searched Ovid MEDLINE, Ovid EMBASE, Cochrane Library, Science Citation Index (Web of Science) and ClinicalTrials.gov for the following end points: biochemical failure (BF), overall survival (OS), prostate cancer-specific survival (PCSS) and side effects. The meta-analysis was performed by using Review Manager 5.2 and Stata version 12.0 software packages. Results were expressed as the odds ratio (OR) with the corresponding 95 % confidence interval (CI).
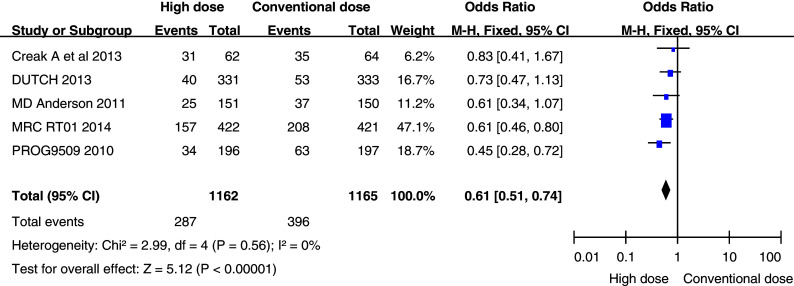
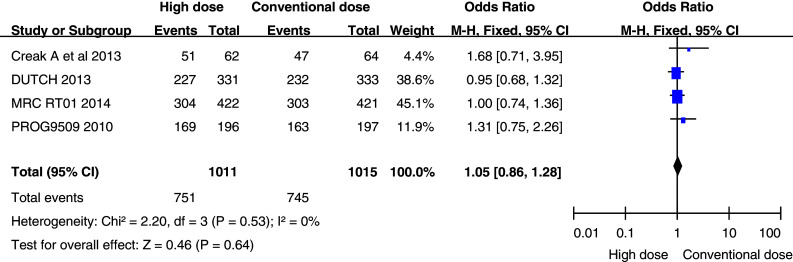
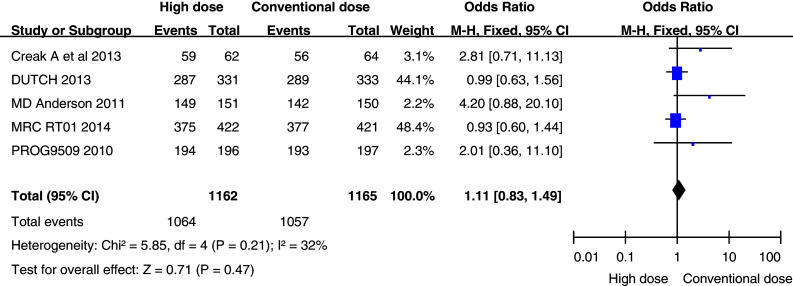
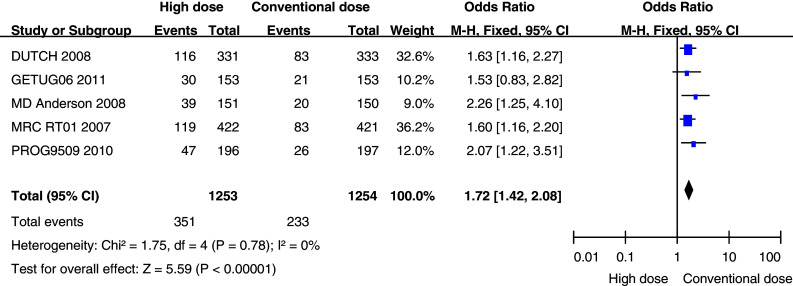
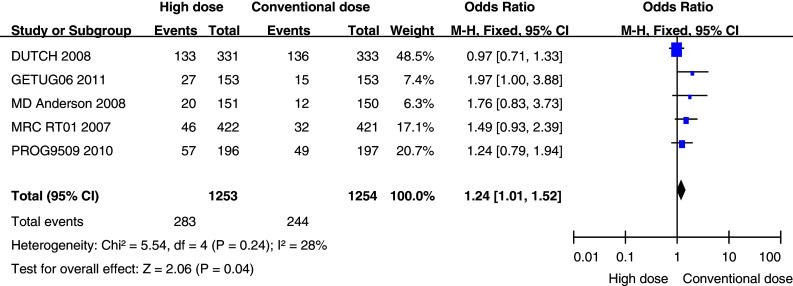
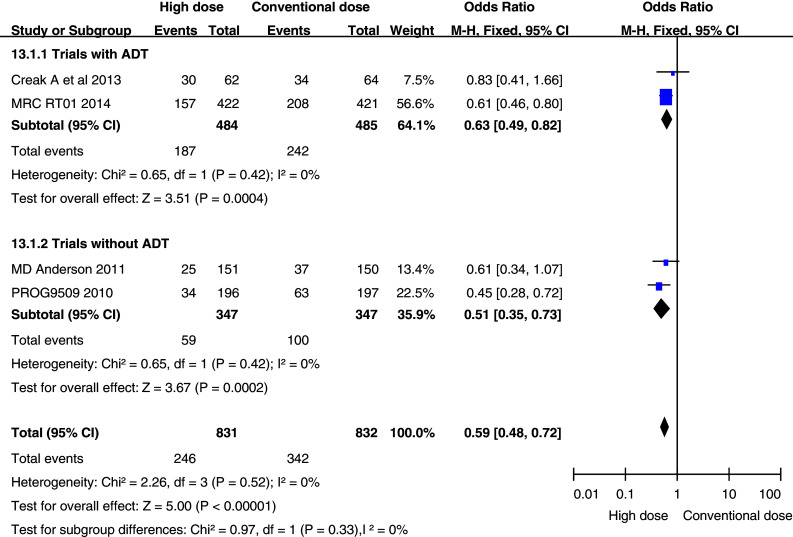
Results: Six randomized controlled trials, with a total population of 2,822, were eligible. In terms of 10-year efficacy relative to CDRT, the HDRT was associated with almost an equivalent OS (73.4 vs. 74.3 %, OR 1.05, 95 % CI 0.86-1.28; p = 0.64) and PCSS (90.7 vs. 91.6 %, OR 1.11, 95 % CI 0.83-1.49; p = 0.47), but a significant decrease in the BF (34.0 vs. 24.7 %, OR 0.61, 95 % CI 0.51-0.74; p < 0.00001). In terms of toxicity, HDRT significantly increased the late Grade 2 or higher (G ≥ 2) gastrointestinal toxicity (28.0 vs. 18.6 %, OR 1.72, 95 % CI 1.42-2.08; p < 0.00001) and late G ≥ 2 genitourinary (GU) toxicity (22.6 vs. 19.5 %, OR 1.24, 95 % CI 1.01-1.52; p = 0.04). In the subgroup analysis, trials with or without androgen deprivation therapy both had a significant decrease in the BF at 10 years. With regard to quality of life, there was no significant difference between HDRT and CDRT (p > 0.05).
Conclusion: This was the first meta-analysis of trials with long-term follow-up to indicate that HDRT is superior to CDRT in terms of preventing BF in localized prostate cancer patients. However, this advantage did not translate into an improvement in OS and PCSS. This was also the first meta-analysis to suggest that the HDRT in three-dimensional conformal radiotherapy (3D-CRT) significantly increases the late G ≥ 2 GU toxicity. Thus, the dose escalation in 3D-CRT should be discreetly used in the treatment of prostate cancer due to the increase in late toxicities.
Figures
References
-
- Al-Mamgani A, van Putten WLJ, Heemsbergen WD et al (2008) Update of Dutch multicenter dose-escalation trial of radiotherapy for localized prostate cancer. Int J Radiat Oncol Biol Phys 72:980–988 - PubMed
-
- Al-Mamgani A, van Puten WLJ, van der Wielen GJ et al (2011) Dose escalation and quality of life in patients with localized prostate cancer treated with radiotherapy: long-term results of the Dutch randomized dose-escalation trial (CKTO 96-10 trial). Int J Radiat Oncol Biol Phys 79:1004–1012 - PubMed
-
- Beckendorf V, Guerif S, Le Prise E et al (2011) 70 Gy versus 80 Gy in localized prostate cancer: 5-year results of GETUG 06 randomized trial. Int J Radiat Oncol Biol Phys 80(4):1056–1063 - PubMed
-
- Begg CB, Mazumdar M (1994) Operating characteristics of a rank correlation test for publication bias. Biometrics 50:1088–1101 - PubMed
-
- Cancer Research UK Prostate cancer statistics—key facts (2011). http://infocancerresearchuk.org/cancerstats/keyfacts/prostate-cancer/
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
