

Intensity modulated radiotherapy (IMRT) with concurrent chemotherapy as definitive treatment of locally advanced esophageal cancer
- PMID: 25175056
- PMCID: PMC4156653
- DOI: 10.1186/1748-717X-9-191
Intensity modulated radiotherapy (IMRT) with concurrent chemotherapy as definitive treatment of locally advanced esophageal cancer
Abstract
Background: To report our experience with increased dose intensity-modulated radiation and concurrent systemic chemotherapy as definitive treatment of locally advanced esophageal cancer.
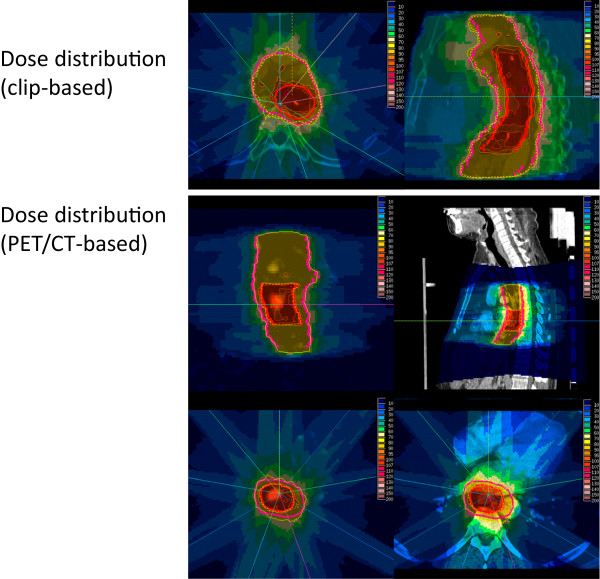
Patients and methods: We analyzed 27 consecutive patients with histologically proven esophageal cancer, who were treated with increased-dose IMRT as part of their definitive therapy. The majority of patients had T3/4 and/or N1 disease (93%). Squamous cell carcinoma was the dominating histology (81%). IMRT was delivered in step-and-shoot technique in all patients using an integrated boost concept. The boost volume was covered with total doses of 56-60 Gy (single dose 2-2.14 Gy), while regional nodal regions received 50.4 Gy (single dose 1.8 Gy) in 28 fractions. Concurrent systemic therapy was scheduled in all patients and administered in 26 (96%). 17 patients received additional adjuvant systemic therapy. Loco-regional control, progression-free and overall survival as well as acute and late toxicities were retrospectively analyzed. In addition, quality of life was prospectively assessed according to the EORTC QLQs (QLQ-OG25, QLQ-H&N35 and QLQ-C30).
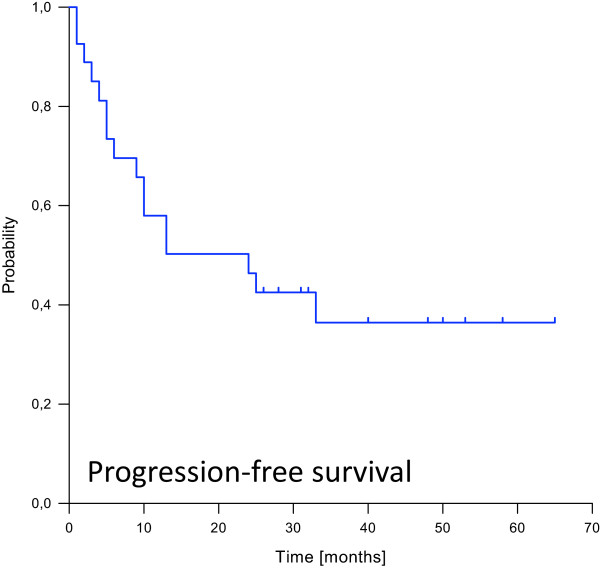
Results: Radiotherapy was completed as planned in all but one patient (96%), and 21 patients received more than 80% of the planned concurrent systemic therapy. We observed ten locoregional failures, transferring into actuarial 1-, 2- and 3-year-locoregional control rates of 77%, 65% and 48%. Seven patients developed distant metastases, mainly to the lung (71%). The actuarial 1-, 2- and 3-year-disease free survival rates were 58%, 48% and 36%, and overall survival rates were 82%, 61% and 56%. The concept was well tolerated, both in the clinical objective examination and also according to the subjective answers to the QLQ questionnaire. 14 patients (52%) suffered from at least one acute CTC grade 3/4 toxicity, mostly hematological side effects or dysphagia. Severe late toxicities were reported in 6 patients (22%), mostly esophageal strictures and ulcerations. Severe side effects to skin, lung and heart were rare.
Conclusion: IMRT with concurrent systemic therapy in the definitive treatment of esophageal cancer using an integrated boost concept with doses up to 60 Gy is feasible and yields good results with acceptable acute and late overall toxicity and low side effects to skin, lung and heart.
Figures


Similar articles
-
Tolerance and efficacy of dose escalation using IMRT combined with chemotherapy for unresectable esophageal carcinoma: Long-term results of 51 patients.Cancer Radiother. 2020 Apr;24(2):88-92. doi: 10.1016/j.canrad.2020.01.006. Epub 2020 Mar 7. Cancer Radiother. 2020. PMID: 32156457
-
Intensity modulated radiotherapy (IMRT) combined with concurrent but not adjuvant chemotherapy in primary nasopharyngeal cancer - a retrospective single center analysis.Radiat Oncol. 2013 Jan 24;8:20. doi: 10.1186/1748-717X-8-20. Radiat Oncol. 2013. PMID: 23347410 Free PMC article. Clinical Trial.
-
IMRT-SIB with concurrent and neo-adjuvant platinum-based chemotherapy for locally advanced head and neck squamous cell cancer: analysis of clinical outcomes in a retrospective series of a single institution.Tumori. 2014 Nov-Dec;100(6):652-9. doi: 10.1700/1778.19272. Tumori. 2014. PMID: 25688499
-
Clinical experience of SIB-IMRT in anal cancer and selective literature review.Radiat Oncol. 2014 Sep 8;9:199. doi: 10.1186/1748-717X-9-199. Radiat Oncol. 2014. PMID: 25199879 Free PMC article. Review.
-
Treatment outcomes after definitive radio(chemo)therapy for 17 lacrimal sac squamous cell carcinoma.Br J Radiol. 2020 Nov 1;93(1115):20190633. doi: 10.1259/bjr.20190633. Epub 2020 Oct 6. Br J Radiol. 2020. PMID: 32970475 Free PMC article. Review.
Cited by
-
Radiobiological evaluation of simultaneously dose-escalated versus non-escalated intensity-modulated radiation therapy for patients with upper thoracic esophageal cancer.Onco Targets Ther. 2017 Apr 19;10:2209-2217. doi: 10.2147/OTT.S132388. eCollection 2017. Onco Targets Ther. 2017. PMID: 28458564 Free PMC article.
-
Advances in radiotherapy in the treatment of esophageal cancer.World J Clin Oncol. 2025 Mar 24;16(3):102872. doi: 10.5306/wjco.v16.i3.102872. World J Clin Oncol. 2025. PMID: 40130058 Free PMC article.
-
[Normal tissue: radiosensitivity, toxicity, consequences for planning].Radiologe. 2018 Aug;58(8):746-753. doi: 10.1007/s00117-018-0430-4. Radiologe. 2018. PMID: 29992402 Review. German.
-
Geriatric Radiation Oncology: What We Know and What Can We Do Better?Clin Interv Aging. 2023 May 4;18:689-711. doi: 10.2147/CIA.S365495. eCollection 2023. Clin Interv Aging. 2023. PMID: 37168037 Free PMC article. Review.
-
Thoracic Vertebral Body Irradiation Contributes to Acute Hematologic Toxicity During Chemoradiation Therapy for Non-Small Cell Lung Cancer.Int J Radiat Oncol Biol Phys. 2016 Jan 1;94(1):147-154. doi: 10.1016/j.ijrobp.2015.09.022. Epub 2015 Sep 25. Int J Radiat Oncol Biol Phys. 2016. PMID: 26700708 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
