

Pediatric cochlear implantation: an update
- PMID: 25179127
- PMCID: PMC4282008
- DOI: 10.1186/s13052-014-0072-8
Pediatric cochlear implantation: an update
Abstract
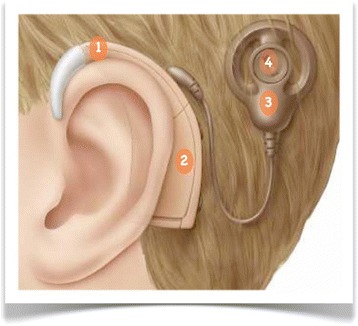
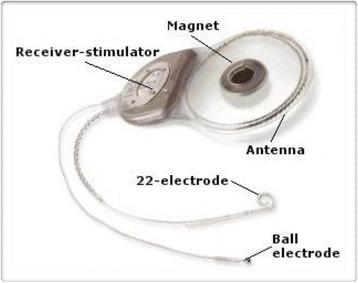
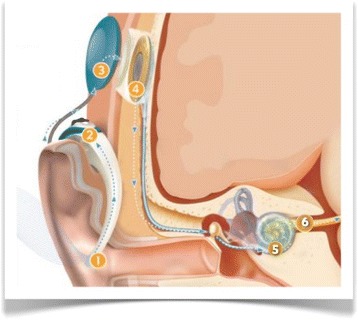
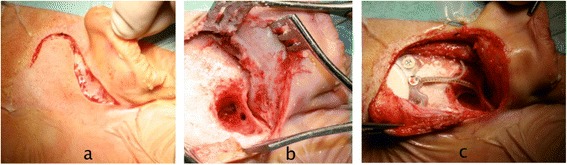
Deafness in pediatric age can adversely impact language acquisition as well as educational and social-emotional development. Once diagnosed, hearing loss should be rehabilitated early; the goal is to provide the child with maximum access to the acoustic features of speech within a listening range that is safe and comfortable. In presence of severe to profound deafness, benefit from auditory amplification cannot be enough to allow a proper language development. Cochlear implants are partially implantable electronic devices designed to provide profoundly deafened patients with hearing sensitivity within the speech range. Since their introduction more than 30 years ago, cochlear implants have improved their performance to the extent that are now considered to be standard of care in the treatment of children with severe to profound deafness. Over the years patient candidacy has been expanded and the criteria for implantation continue to evolve within the paediatric population. The minimum age for implantation has progressively reduced; it has been recognized that implantation at a very early age (12-18 months) provides children with the best outcomes, taking advantage of sensitive periods of auditory development. Bilateral implantation offers a better sound localization, as well as a superior ability to understand speech in noisy environments than unilateral cochlear implant. Deafened children with special clinical situations, including inner ear malformation, cochlear nerve deficiency, cochlear ossification, and additional disabilities can be successfully treated, even thogh they require an individualized candidacy evaluation and a complex post-implantation rehabilitation. Benefits from cochlear implantation include not only better abilities to hear and to develop speech and language skills, but also improved academic attainment, improved quality of life, and better employment status. Cochlear implants permit deaf people to hear, but they have a long way to go before their performance being comparable to that of the intact human ear; researchers are looking for more sophisticated speech processing strategies as well as a more efficient coupling between the electrodes and the cochlear nerve with the goal of dramatically improving the quality of sound of the next generation of implants.
Figures
References
-
- Ramsden JD, Gordon K, Aschendorff A, Borucki L, Bunne M, Burdo S, Garabedian N, Grolman W, Irving R, Lesinski-Schiedat A, Loundon N, Manrique M, Martin J, Raine C, Wouters J, Papsin BC. European bilateral pediatric cochlear implant forum consensus statement. Otol Neurotol. 2012;33:346–350. doi: 10.1097/MAO.0b013e3182536ae2. - DOI - PubMed
-
- Almond M, Brown DJ. The pathology and etiology of sensorineural hearing loss and implications for cochlear implantation. In: Niparko JK, editor. Cochlear implants: principles & practice. 2. Philadelphia: Lippincott Williams & Wilkins; 2009. pp. 43–81.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
