

A randomized pilot trial of remote ischemic preconditioning in heart failure with reduced ejection fraction
- PMID: 25181050
- PMCID: PMC4152122
- DOI: 10.1371/journal.pone.0105361
A randomized pilot trial of remote ischemic preconditioning in heart failure with reduced ejection fraction
Abstract
Background: Remote ischemic preconditioning (RIPC) induced by transient limb ischemia confers multi-organ protection and improves exercise performance in the setting of tissue hypoxia. We aimed to evaluate the effect of RIPC on exercise capacity in heart failure patients.
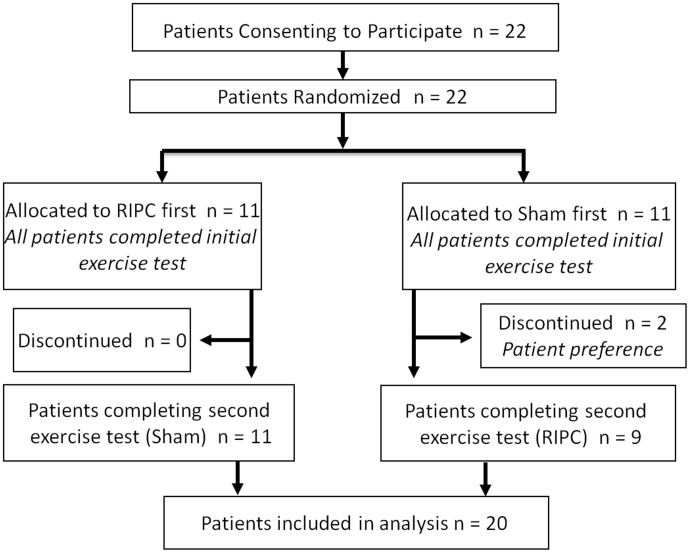
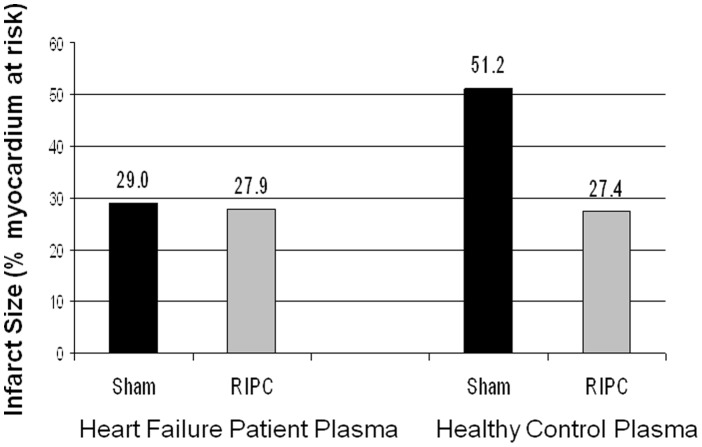
Methods: We performed a randomized crossover trial of RIPC (4×5-minutes limb ischemia) compared to sham control in heart failure patients undergoing exercise testing. Patients were randomly allocated to either RIPC or sham prior to exercise, then crossed over and completed the alternate intervention with repeat testing. The primary outcome was peak VO2, RIPC versus sham. A mechanistic substudy was performed using dialysate from study patient blood samples obtained after sham and RIPC. This dialysate was used to test for a protective effect of RIPC in a mouse heart Langendorff model of infarction. Mouse heart infarct size with RIPC or sham dialysate exposure was also compared with historical control data.
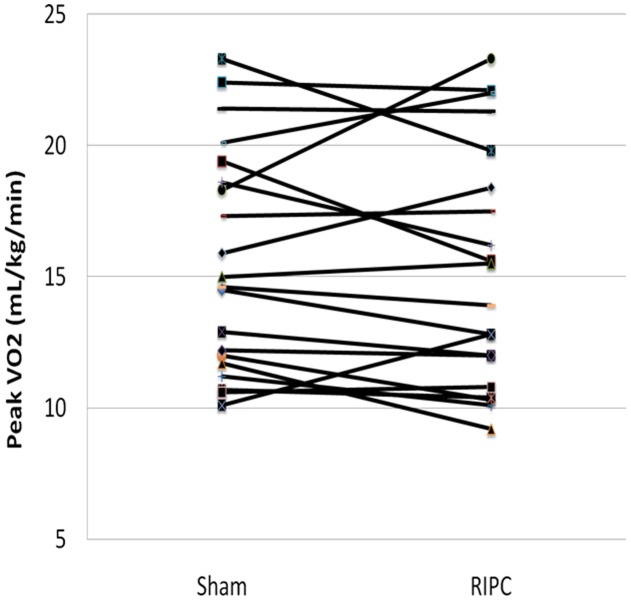
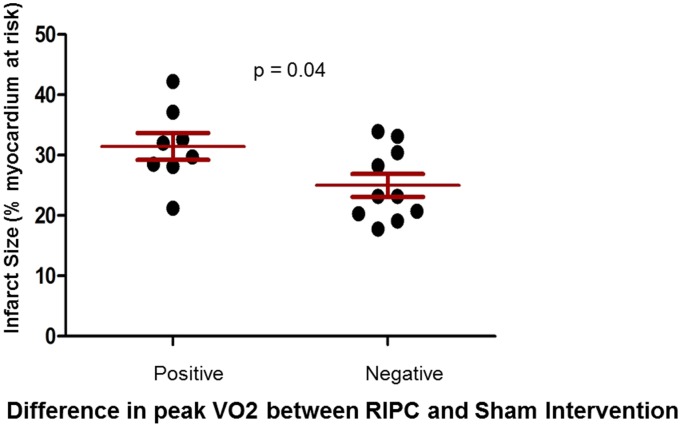
Results: Twenty patients completed the study. RIPC was not associated with improvements in peak VO2 (15.6+/-4.2 vs 15.3+/-4.6 mL/kg/min; p = 0.53, sham and RIPC, respectively). In our Langendorff sub-study, infarct size was similar between RIPC and sham dialysate groups from our study patients, but was smaller than expected compared to healthy controls (29.0%, 27.9% [sham, RIPC] vs 51.2% [controls]. We observed less preconditioning among the subgroup of patients with increased exercise performance following RIPC (p<0.04).
Conclusion: In this pilot study of RIPC in heart failure patients, RIPC was not associated with improvements in exercise capacity overall. However, the degree of effect of RIPC may be inversely related to the degree of baseline preconditioning. These data provide the basis for a larger randomized trial to test the potential benefits of RIPC in patients with heart failure.
Trial registration: ClinicalTrials.gov +++++NCT01128790.
Conflict of interest statement
Figures
References
-
- McElroy PA, Janicki JS, Weber KT (1988) Cardiopulmonary exercise testing in congestive heart failure. Am J Cardiol 62: 35A–40A. - PubMed
-
- Mancini DM, Eisen H, Kussmaul W, Mull R, Edmunds LH Jr, et al. (1991) Value of peak exercise oxygen consumption for optimal timing of cardiac transplantation in ambulatory patients with heart failure. Circulation 83: 778–86. - PubMed
-
- Pardaens K, Van Cleemput J, Vanhaecke J, Fagard RH (2000) Peak oxygen uptake better predicts outcome than submaximal respiratory data in heart transplant candidates. Circulation 101: 1152–57. - PubMed
-
- O'Neill JO, Young JB, Pothier CE, Lauer MS (2005) Peak oxygen consumption as a predictor of death in patients with heart failure receiving beta-blockers. Circulation 111: 2313–18. - PubMed
-
- Aaronson KD, Schwartz JS, Chen TM, Wong KL, Goin JE, et al. (1997) Development and prospective validation of a clinical index to predict survival in ambulatory patients referred for cardiac transplant evaluation. Circulation 95: 2660–67. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
