

Histoplasma capsulatum endocarditis: multicenter case series with review of current diagnostic techniques and treatment
- PMID: 25181311
- PMCID: PMC4602453
- DOI: 10.1097/MD.0000000000000034
Histoplasma capsulatum endocarditis: multicenter case series with review of current diagnostic techniques and treatment
Abstract
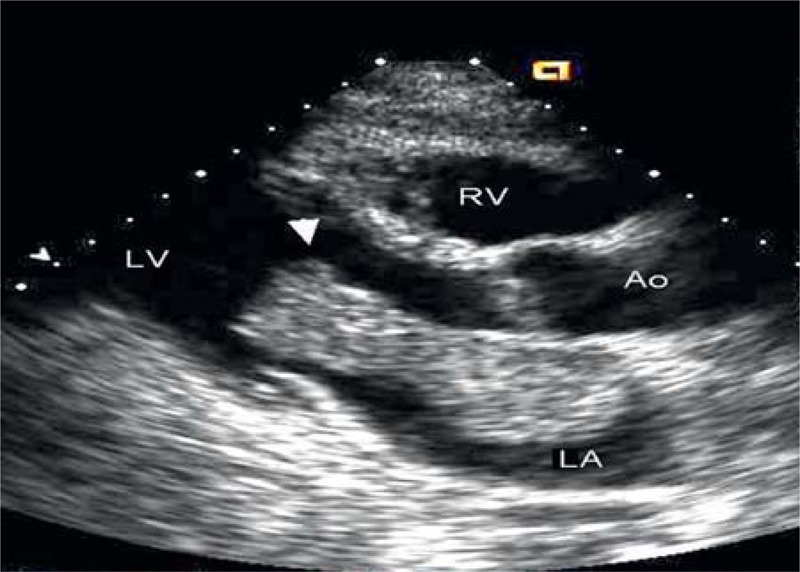
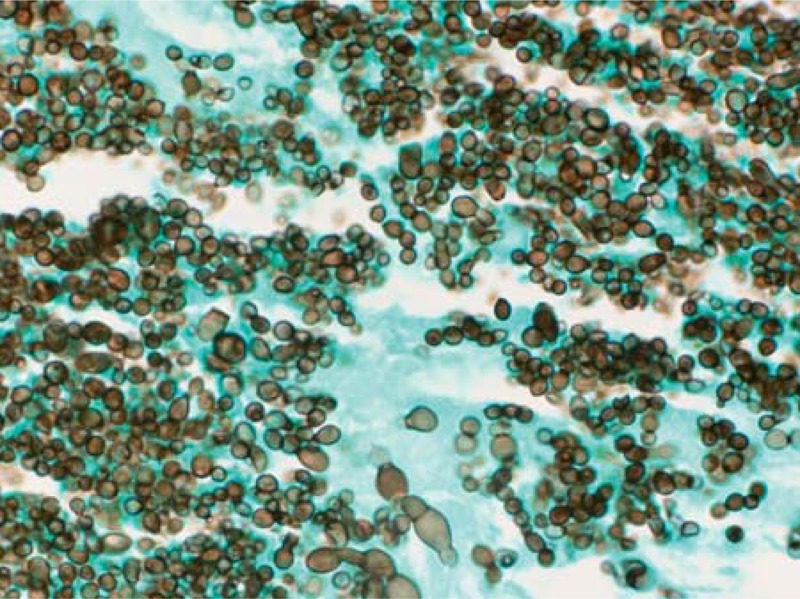
Infective endocarditis is an uncommon manifestation of infection with Histoplasma capsulatum. The diagnosis is frequently missed, and outcomes historically have been poor. We present 14 cases of Histoplasma endocarditis seen in the last decade at medical centers throughout the United States. All patients were men, and 10 of the 14 had an infected prosthetic aortic valve. One patient had an infected left atrial myxoma. Symptoms were present a median of 7 weeks before the diagnosis was established. Blood cultures yielded H. capsulatum in only 6 (43%) patients. Histoplasma antigen was present in urine and/or serum in all but 3 of the patients and provided the first clue to the diagnosis of histoplasmosis for several patients. Antibody testing was positive for H. capsulatum in 6 of 8 patients in whom the test was performed. Eleven patients underwent surgery for valve replacement or myxoma removal. Large, friable vegetations were noted at surgery in most patients, confirming the preoperative transesophageal echocardiography findings. Histopathologic examination of valve tissue and the myxoma revealed granulomatous inflammation and large numbers of organisms in most specimens. Four of the excised valves and the atrial myxoma showed a mixture of both yeast and hyphal forms on histopathology. A lipid formulation of amphotericin B, administered for a median of 29 days, was the initial therapy in 11 of the 14 patients. This was followed by oral itraconazole therapy, in all but 2 patients. The length of itraconazole suppressive therapy ranged from 11 months to lifelong administration. Three patients (21%) died within 3 months of the date of diagnosis. All 3 deaths were in patients who had received either no or minimal (1 day and 1 week) amphotericin B.
Conflict of interest statement
Financial support and conflicts of interest: L.J.W. is President and Director of MiraVista Diagnostics. The other authors have no funding or conflicts of interest to disclose.
Figures


References
-
- Baddour LM, Wilson WR, Bayer Fowler ASVG, et al. Infective endocarditis: diagnosis, antimicrobial therapy, and management of complications: a statement for healthcare professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, and the Councils on Clinical Cardiology, Stroke, and Cardiovascular Surgery and Anesthesia, American Heart Association: endorsed by the Infectious Diseases Society of America. Circulation. 2005;111:e394–e434. - PubMed
-
- Balajee SA, Sigler L, Brandt ME. DNA and the classical way: identification of medically important molds in the 21st century. Med Mycol. 2007;45:475–490. - PubMed
-
- Bhatti S, Vilenski L, Tight R. Smego RA Jr. Histoplasma endocarditis: clinical and mycologic features and outcomes. J Infect. 2005;51:2–9. - PubMed
-
- Bialek R, Ernst F, Dietz K, et al. Comparison of staining methods and a nested PCR assay to detect Histoplasma capsulatum in tissue sections. Am J Clin Pathol. 2002;117:597–603. - PubMed
-
- Binford CH. Histoplasmosis: tissue reactions and morphologic variations of fungus. Am J Clin Pathol. 1955;25:25–36. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
