

Diffusion-weighted imaging in cancer: physical foundations and applications of restriction spectrum imaging
- PMID: 25183788
- PMCID: PMC4155409
- DOI: 10.1158/0008-5472.CAN-13-3534
Diffusion-weighted imaging in cancer: physical foundations and applications of restriction spectrum imaging
Erratum in
- Cancer Res. 2014 Nov 15;74(22):6733. McDonald, Carrie R [corrected to McDonald, Carrie];Kaine, Christopher J [corrected to Kane, Christopher J]
Abstract
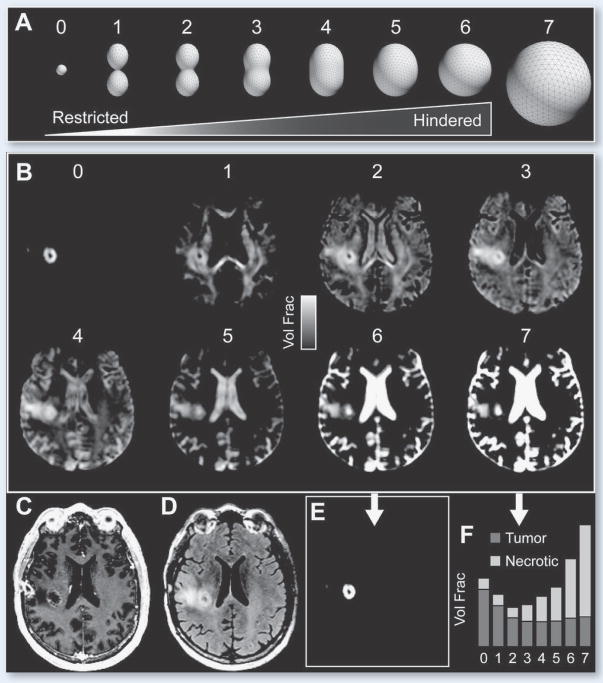
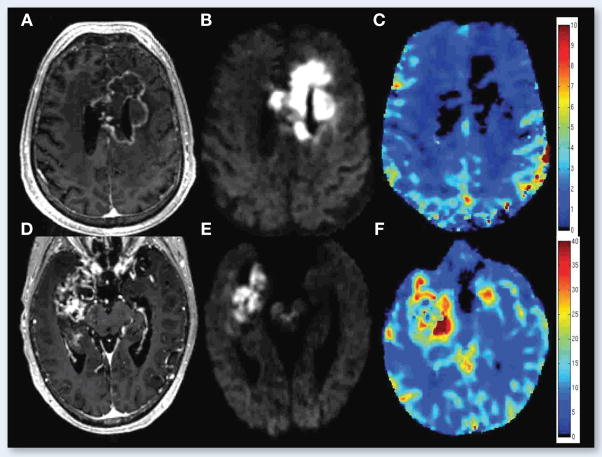
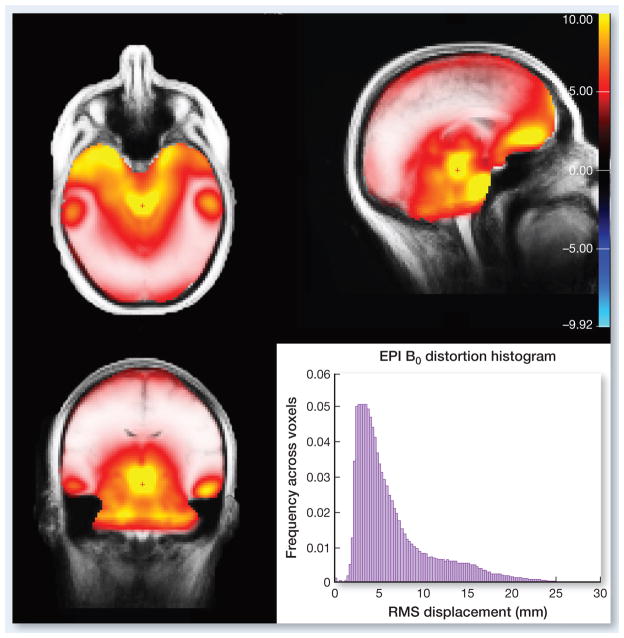
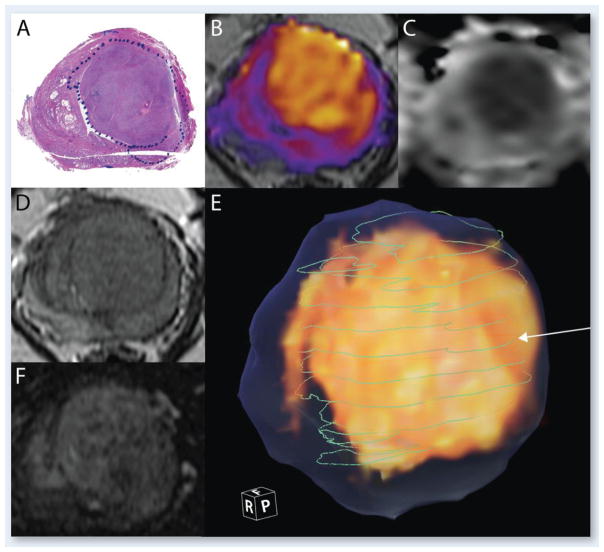
Diffusion-weighted imaging (DWI) has been at the forefront of cancer imaging since the early 2000s. Before its application in clinical oncology, this powerful technique had already achieved widespread recognition due to its utility in the diagnosis of cerebral infarction. Following this initial success, the ability of DWI to detect inherent tissue contrast began to be exploited in the field of oncology. Although the initial oncologic applications for tumor detection and characterization, assessing treatment response, and predicting survival were primarily in the field of neurooncology, the scope of DWI has since broadened to include oncologic imaging of the prostate gland, breast, and liver. Despite its growing success and application, misconceptions about the underlying physical basis of the DWI signal exist among researchers and clinicians alike. In this review, we provide a detailed explanation of the biophysical basis of diffusion contrast, emphasizing the difference between hindered and restricted diffusion, and elucidating how diffusion parameters in tissue are derived from the measurements via the diffusion model. We describe one advanced DWI modeling technique, called restriction spectrum imaging (RSI). This technique offers a more direct in vivo measure of tumor cells, due to its ability to distinguish separable pools of water within tissue based on their intrinsic diffusion characteristics. Using RSI as an example, we then highlight the ability of advanced DWI techniques to address key clinical challenges in neurooncology, including improved tumor conspicuity, distinguishing actual response to therapy from pseudoresponse, and delineation of white matter tracts in regions of peritumoral edema. We also discuss how RSI, combined with new methods for correction of spatial distortions inherent in diffusion MRI scans, may enable more precise spatial targeting of lesions, with implications for radiation oncology and surgical planning. See all articles in this Cancer Research section, "Physics in Cancer Research."
©2014 American Association for Cancer Research.
Conflict of interest statement
Conflicts of interest: None of the authors have any personal or institutional financial interest in drugs, materials, or devices described in this submission.
Figures





References
-
- Sugahara T, Korogi Y, Kochi M, Ikushima I, Shigematu Y, Hirai T, et al. Usefulness of diffusion-weighted MRI with echo-planar technique in the evaluation of cellularity in gliomas. J Magn Reson Imaging. 1999;9:53–60. - PubMed
-
- Chen J, Xia J, Zhou YC, Xia LM, Zhu WZ, Zou ML, et al. Correlation between magnetic resonance diffusion weighted imaging and cell density in astrocytoma. Zhonghua Zhong Liu Za Zhi. 2005;27:309–11. - PubMed
-
- Guo AC, Cummings TJ, Dash RC, Provenzale JM. Lymphomas and high-grade astrocytomas: comparison of water diffusibility and histologic characteristics. Radiology. 2002;224:177–83. - PubMed
-
- Server A, Kulle B, Maehlen J, Josefsen R, Schellhorn T, Kumar T, et al. Quantitative apparent diffusion coefficients in the characterization of brain tumors and associated peritumoral edema. Acta Radiol. 2009;50:682–9. - PubMed
