

Techniques of imaging of nodal stations of gastric cancer by endoscopic ultrasound
- PMID: 25184125
- PMCID: PMC4145479
- DOI: 10.4103/2303-9027.138793
Techniques of imaging of nodal stations of gastric cancer by endoscopic ultrasound
Abstract
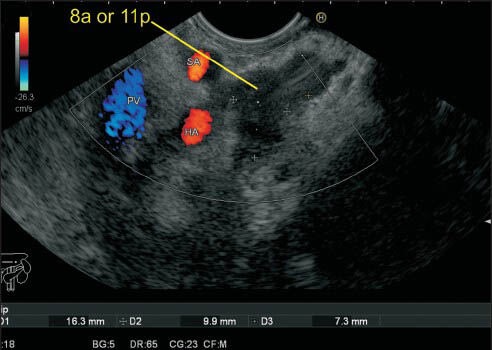
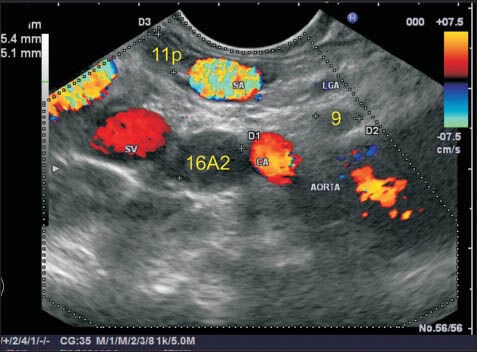
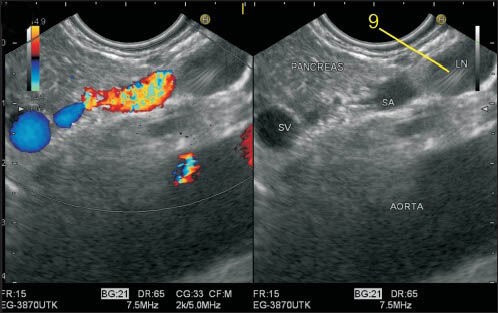
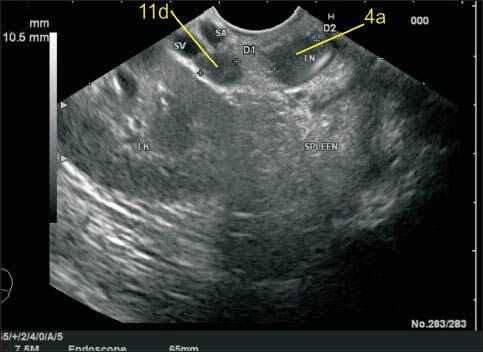
Nodal staging is of crucial importance in the management of gastric cancer (GC). The available modalities of nodal imaging in GC do not provide a high sensitivity and specificity of lymph node status. Comparative study of endoscopic ultrasonography (EUS) and multislice spiral computed tomography in GC has shown greater accuracy of EUS for N staging. EUS is not used routinely in patients with GC as it is not available at all centers, and its accuracy is operator dependent. Standard techniques of identification of nodal station (as suggested by Japanese Research Society for the Study of Gastric Cancer) by EUS have not been described so far. Identification of each nodal station by EUS requires adequate knowledge of anatomy as well as understanding the proper technique to perform EUS. This review presents a method to identify the regional nodal stations of GC by linear EUS and hence will help in appropriate N staging of GC.
Keywords: Endoscopic ultrasound; gastric cancer; lymph node; multidetector spiral computed tomography.
Conflict of interest statement
Figures


References
-
- Park SR, Kim MJ, Ryu KW, et al. Prognostic value of preoperative clinical staging assessed by computed tomography in resectable gastric cancer patients: A viewpoint in the era of preoperative treatment. Ann Surg. 2010;251:428–35. - PubMed
-
- Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011;14:101–12. - PubMed
-
- Kajitani T. The general rules for the gastric cancer study in surgery and pathology. Part I. Clinical classification. Jpn J Surg. 1981;11:127–39. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
