

A Novel multivalent OspA vaccine against Lyme borreliosis is safe and immunogenic in an adult population previously infected with Borrelia burgdorferi sensu lato
- PMID: 25185574
- PMCID: PMC4248771
- DOI: 10.1128/CVI.00406-14
A Novel multivalent OspA vaccine against Lyme borreliosis is safe and immunogenic in an adult population previously infected with Borrelia burgdorferi sensu lato
Abstract
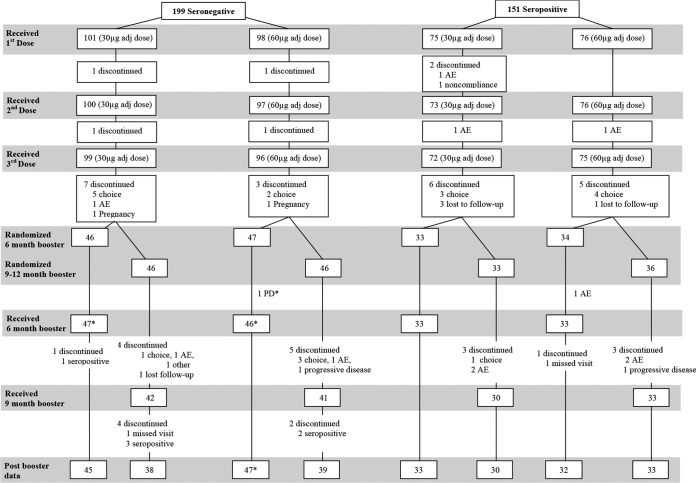
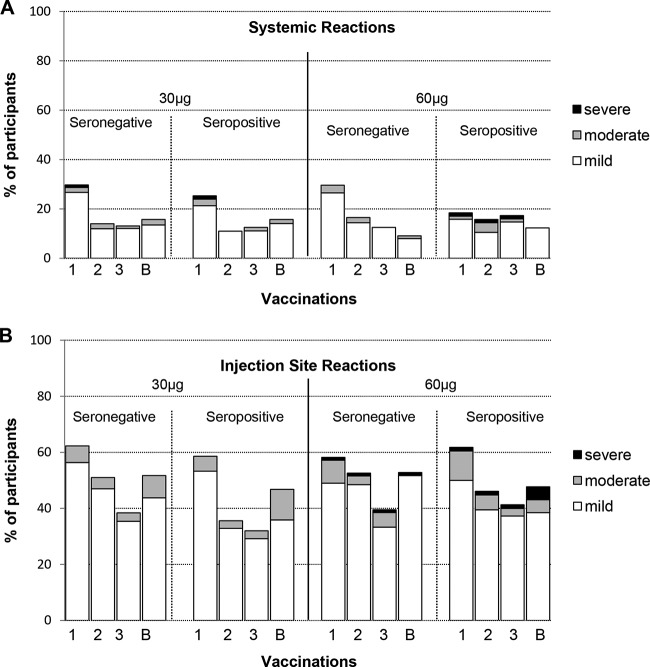
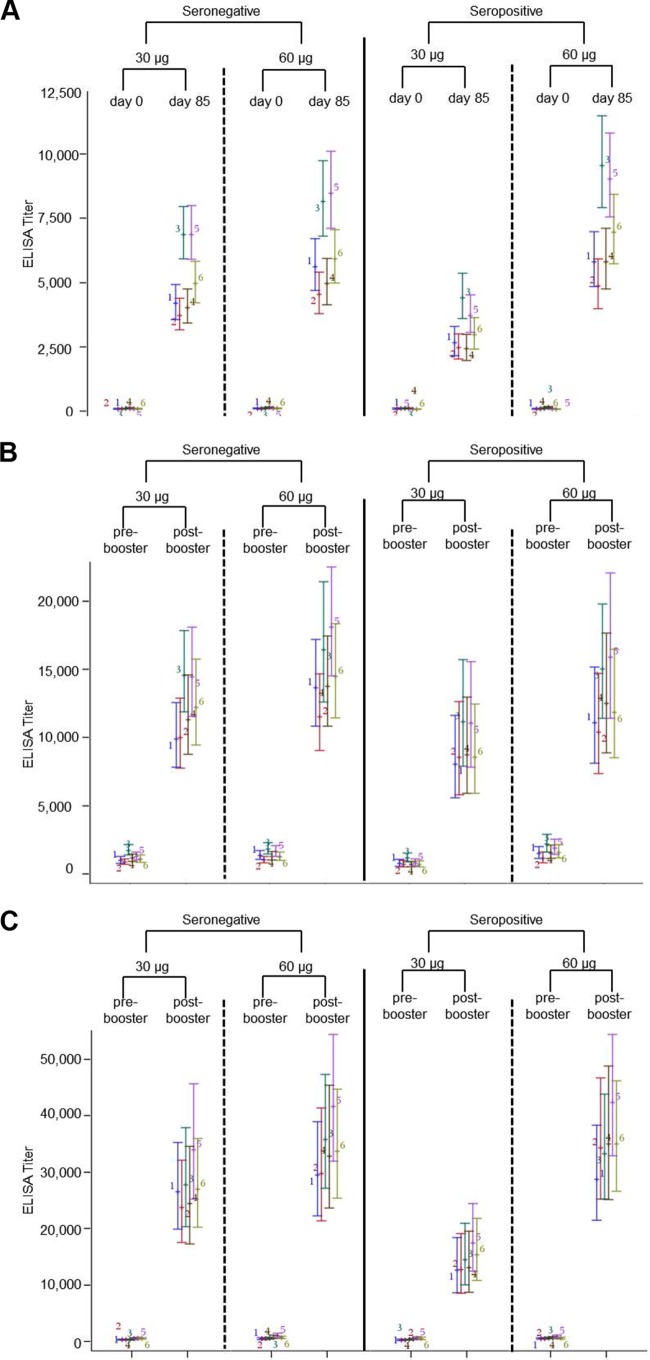
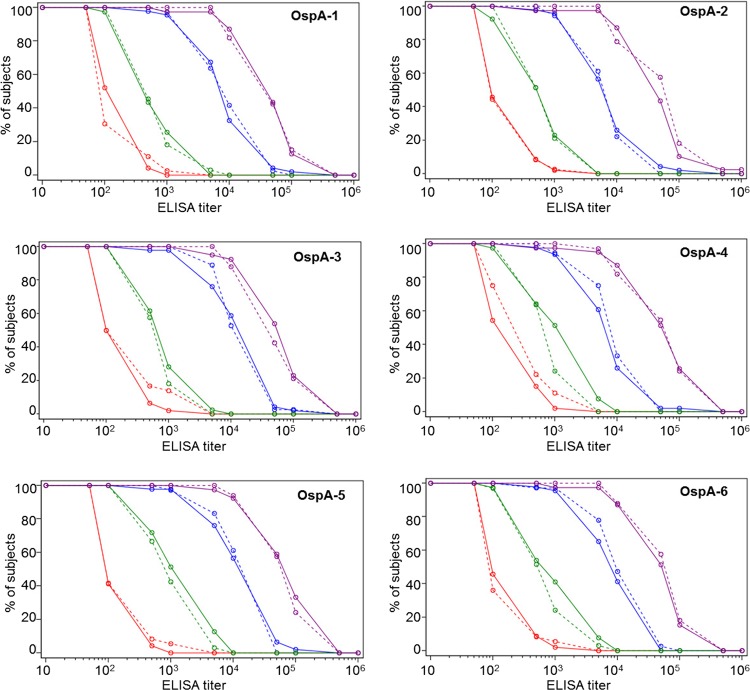
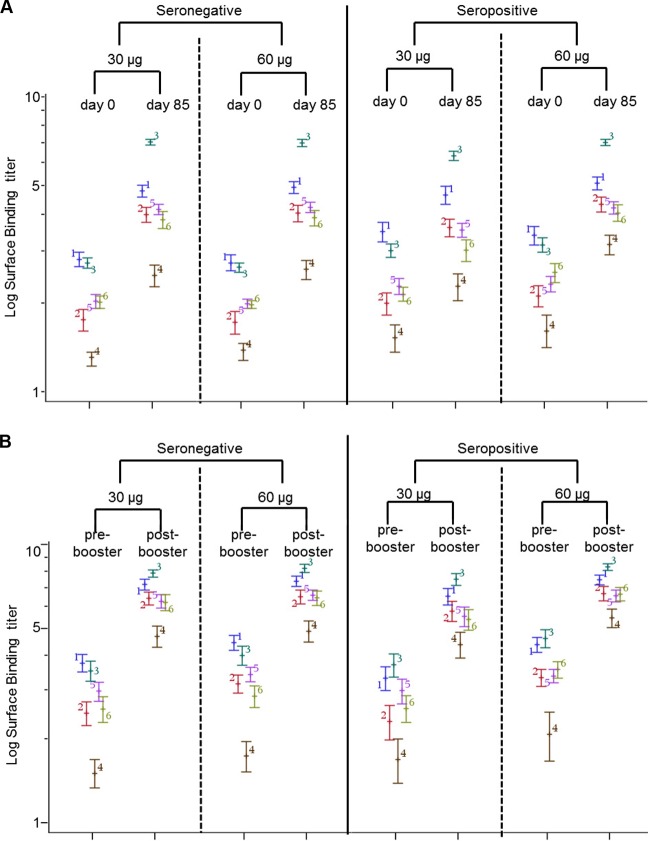
Lyme borreliosis (LB) patients who recover, as well as previously infected asymptomatic individuals, remain vulnerable to reinfection with Borrelia burgdorferi sensu lato. There is limited information available about the use of OspA vaccines in this population. In this study, a randomized double-blind phase I/II trial was performed to investigate the safety and immunogenicity of a novel multivalent OspA vaccine in healthy adults who were either seronegative or seropositive for previous B. burgdorferi sensu lato infection. The participants received three monthly priming immunizations with either 30 μg or 60 μg alum-adjuvanted OspA antigen and a booster vaccination either 6 months or 9 to 12 months after the first immunization. The antibody responses to the six OspA serotypes included in the vaccine were evaluated. Adverse events were predominantly mild and transient and were similar in the seronegative and seropositive populations. Substantial enzyme-linked immunosorbent assay (ELISA) and surface-binding antibody responses against all six OspA antigens were induced after the primary immunization schedule in both populations, and they were substantially increased with both booster schedules. The antibody responses induced by the two doses were similar in the seronegative population, but there was a significant dose response in the seropositive population. These data indicate that the novel multivalent OspA vaccine is well tolerated and immunogenic in individuals previously infected with B. burgdorferi sensu lato. (This study is registered at ClinicalTrials.gov under registration no. NCT01504347.).
Copyright © 2014, American Society for Microbiology. All Rights Reserved.
Figures
References
-
- Steere AC, Livey I. 2012. Lyme disease vaccines, p 1122–1132 In Plotkin SA, Orenstein WA, Offit PA. (ed), Vaccines, 6th ed, Elsevier, Philadelphia, PA.
-
- Lindgren E, Jaenson TGT. 2006. Lyme borreliosis in Europe: influences of climate and climate change, epidemiology, ecology and adaptation measures. World Health Organization Regional Office for Europe, Copenhagen, Denmark: http://www.euro.who.int/document/E89522.pdf.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
