

Increasing hospitalizations in inflammatory bowel disease among children in the United States, 1988-2011
- PMID: 25185689
- PMCID: PMC4762034
- DOI: 10.1097/MIB.0000000000000195
Increasing hospitalizations in inflammatory bowel disease among children in the United States, 1988-2011
Abstract
Background: Our objective was to characterize national trends in inflammatory bowel disease (IBD)-related hospitalizations for children. We hypothesized that over time, improvements in care would be associated with a decrease in hospitalization rates, similar to what has been observed in Canadian children with IBD.
Methods: Retrospective, serial, cross-sectional analysis of annual, nationally representative samples of children with IBD.
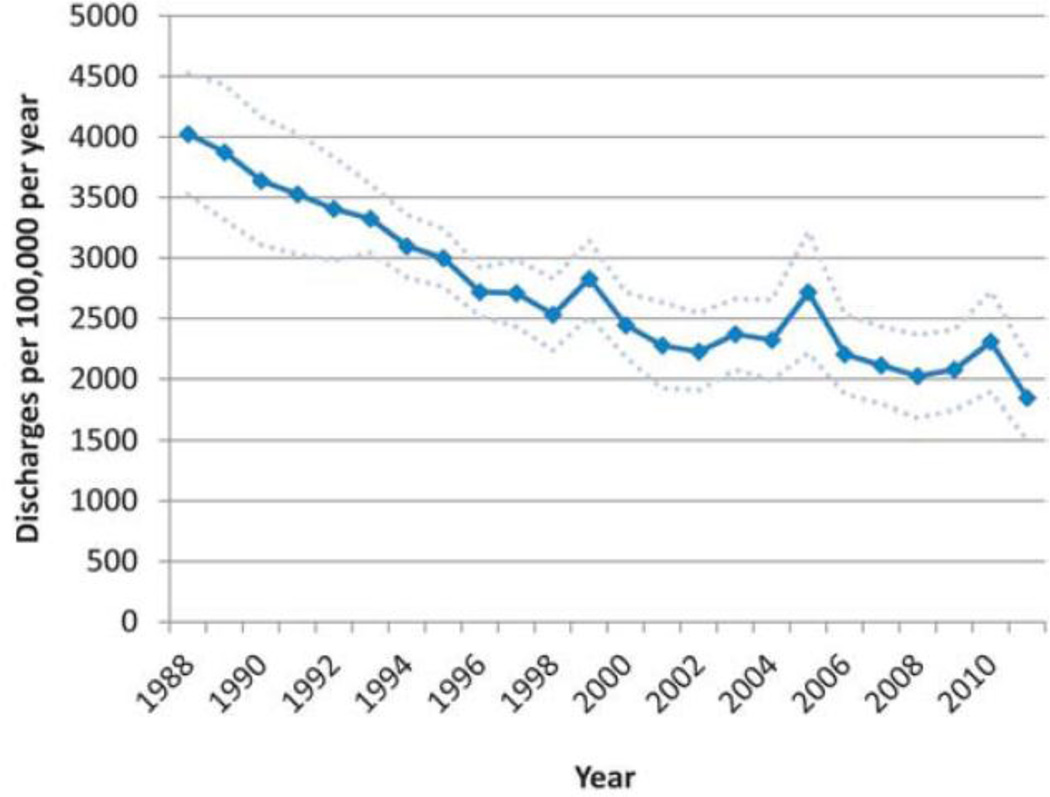
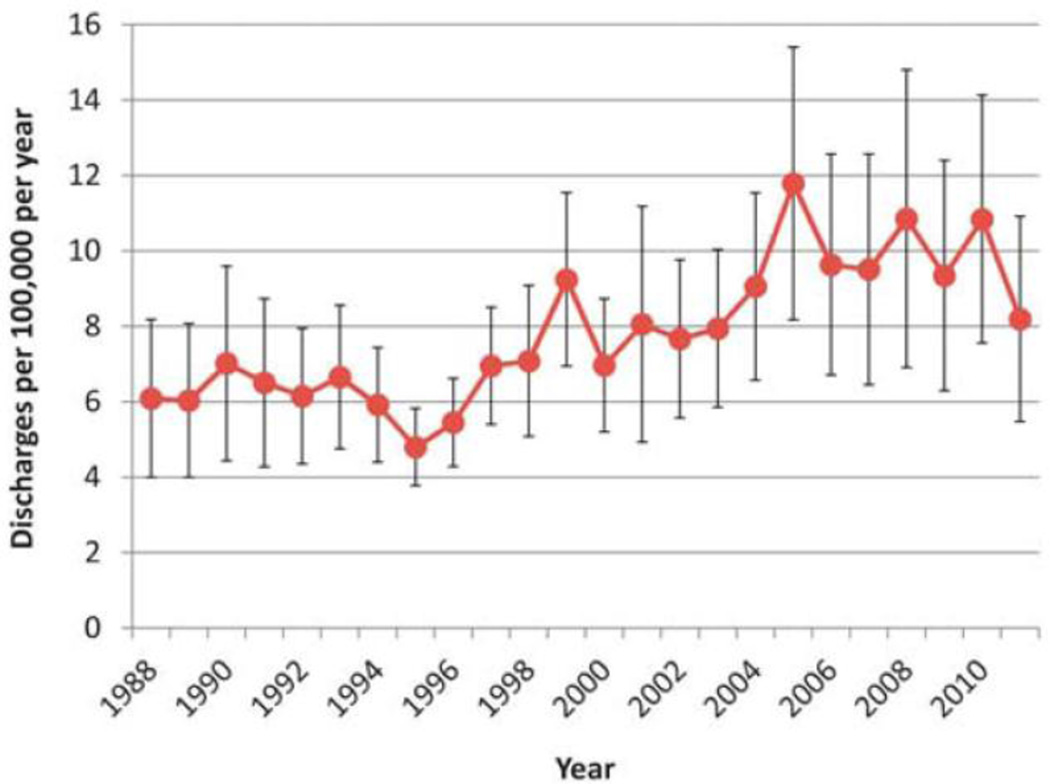
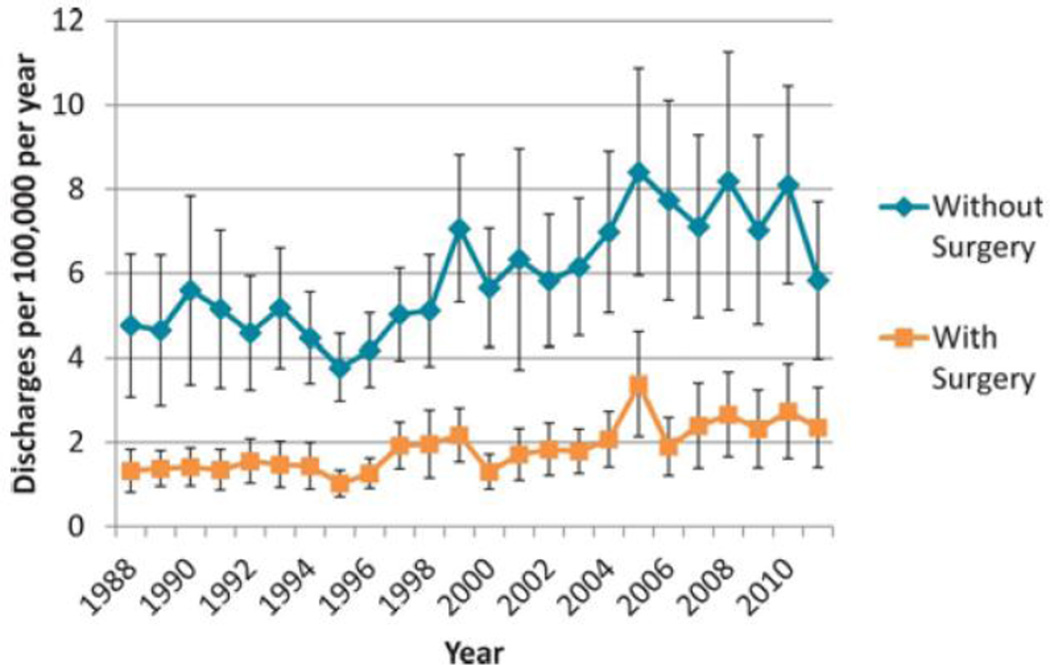
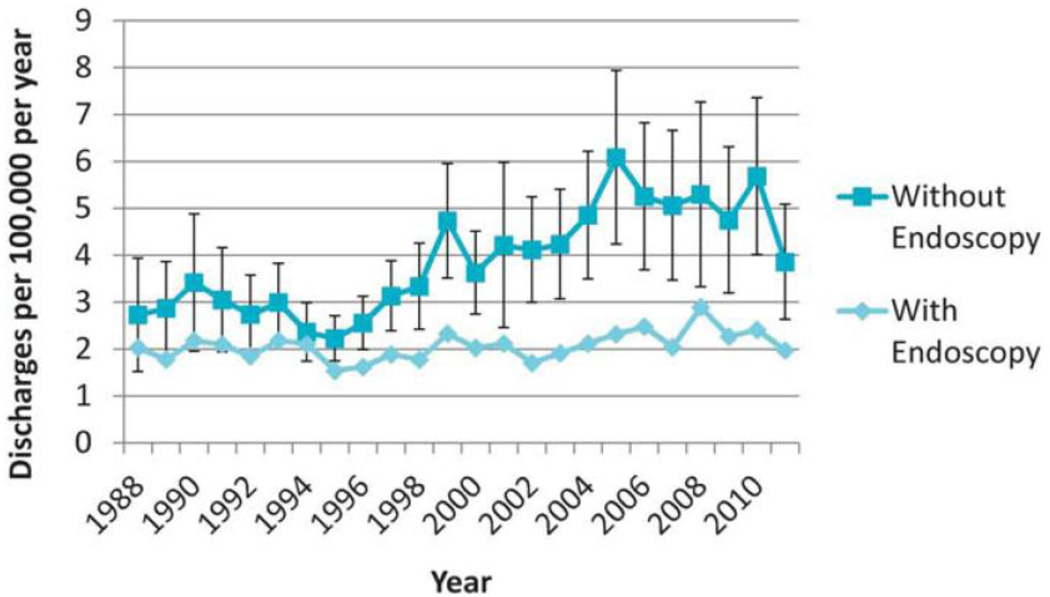
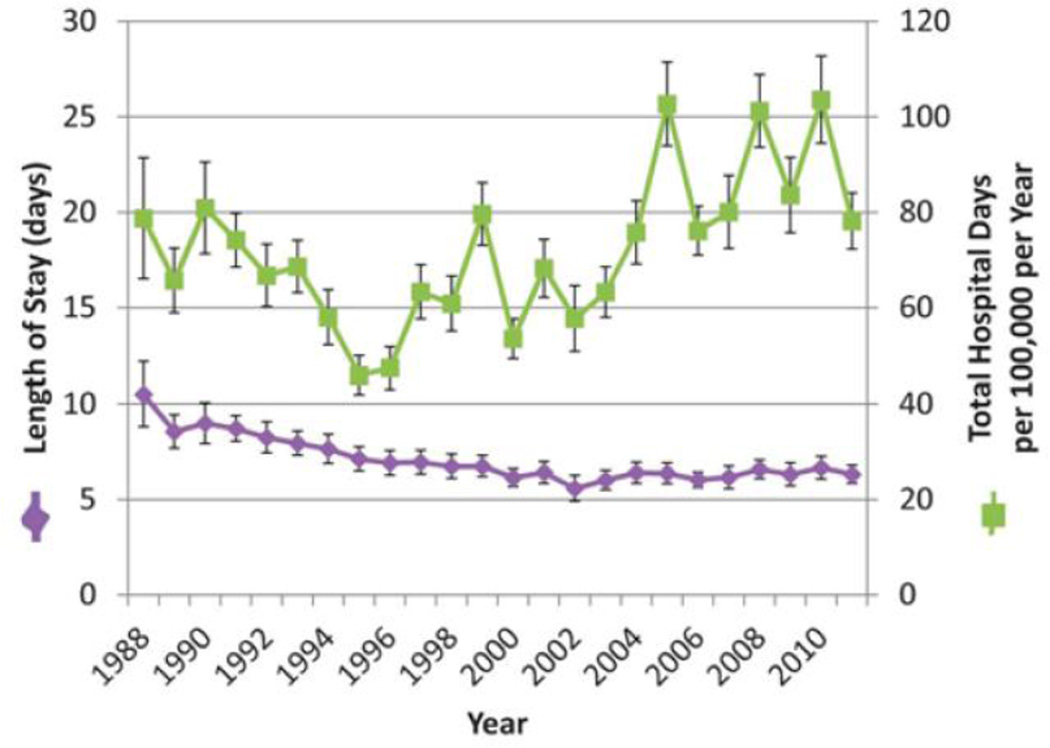
Results: Overall, discharges for all children irrespective of diagnosis decreased from 1988 to 2011 (P for trend <0.001). In contrast, discharges for children with IBD rose over the same time period from 6.1 (95% confidence interval [CI], 4.0-8.2) to 8.2 (95% CI, 5.5-10.9) per 100,000 individuals per year (P for trend <0.001). More of this rise occurred in hospitalizations that did not have IBD-related endoscopy or surgery performed (P for trend <0.001). Although mean length of stay decreased over the study period (P for trend <0.001), total hospital days increased over the latter half of the study with a significant increase over the entire study period (P for trend <0.001).
Conclusions: Contrary to clinically informed hypotheses, nationally representative rates of hospitalization for pediatric patients with IBD have increased since the mid-1990s. This directly contrasts with stable rates over the preceding years. Most of the expansion in hospital care seems to be related to hospitalizations that do not include procedures. Several lines of future research may greatly facilitate a better understanding of the epidemiologic, therapeutic, and health care resource issues at play.
Figures
References
-
- Markowitz J, Grancher K, Kohn N, et al. Immunomodulatory therapy for pediatric inflammatory bowel disease: changing patterns of use, 1990–2000. Am J Gastroenterol. 2002;97:928–932. - PubMed
-
- Nandivada P, Poylin V, Nagle D. Advances in the surgical management of inflammatory bowel disease. Curr Opin Gastroenterol. 2012;28:47–51. - PubMed
-
- Fichera A, Michelassi F. Surgical treatment of Crohn’s disease. J Gastrointest Surg. 2007;11:791–803. - PubMed
-
- Gardiner KR, Dasari BVM. Operative management of small bowel Crohn’s disease. Surg Clin North Am. 2007;87:587–610. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
