

Beyond the time window of intravenous thrombolysis: standing by or by stenting?
- PMID: 25187761
- PMCID: PMC4031767
- DOI: 10.1159/000338389
Beyond the time window of intravenous thrombolysis: standing by or by stenting?
Abstract
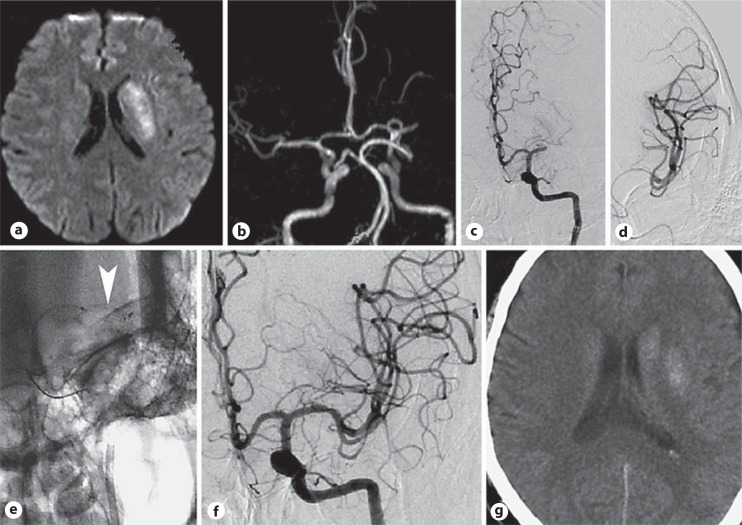
Intravenous administration of tissue plasminogen activator within 4.5 h of symptom onset is presently the 'golden rule' for treating acute ischemic stroke. However, many patients miss the time window and others reject this treatment due to a long list of contraindications. Mechanical embolectomy has recently progressed as a potential alternative for treating patients beyond the time window for IV thrombolysis. In this paper, recent progress in mechanical embolectomy, angioplasty, and stenting in acute stroke is reviewed. Despite worries concerning the long-term clinical outcomes and increased risk of intracranial hemorrhage, favorable clinical outcomes may be achieved after mechanical embolectomy in carefully selected patients even 4.5 h after stroke onset. Potential steps should be prepared and attempted in these patients whose opportunity for recovery will elapse in a flash.
Keywords: Angioplasty; Mechanical embolectomy; Stenting.
Figures
References
-
- Tissue plasminogen activator for acute ischemic stroke – the National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. N Engl J Med. 1995;333:1581–1587. - PubMed
-
- Furlan A, Higashida R, Wechsler L, et al. Intra-arterial prourokinase for acute ischemic stroke: the PROACT II study – a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. JAMA. 1999;282:2003–2011. - PubMed
-
- Bluhmki E, Chamorro A, Davalos A, et al. Stroke treatment with alteplase given 3.0–4.5 h after onset of acute ischaemic stroke (ECASS III): additional outcomes and subgroup analysis of a randomised controlled trial. Lancet Neurol. 2009;8:1095–1102. - PubMed
-
- Reeves MJ, Arora S, Broderick JP, et al. Acute stroke care in the US: results from 4 pilot prototypes of the Paul Coverdell National Acute Stroke Registry. Stroke. 2005;36:1232–1240. - PubMed
-
- Saver JL. Hemorrhage after thrombolytic therapy for stroke: the clinically relevant number needed to harm. Stroke. 2007;38:2279–2283. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
