

Combined endothelin a blockade and chlorthalidone treatment in a rat model of metabolic syndrome
- PMID: 25189702
- PMCID: PMC4201276
- DOI: 10.1124/jpet.114.215566
Combined endothelin a blockade and chlorthalidone treatment in a rat model of metabolic syndrome
Abstract
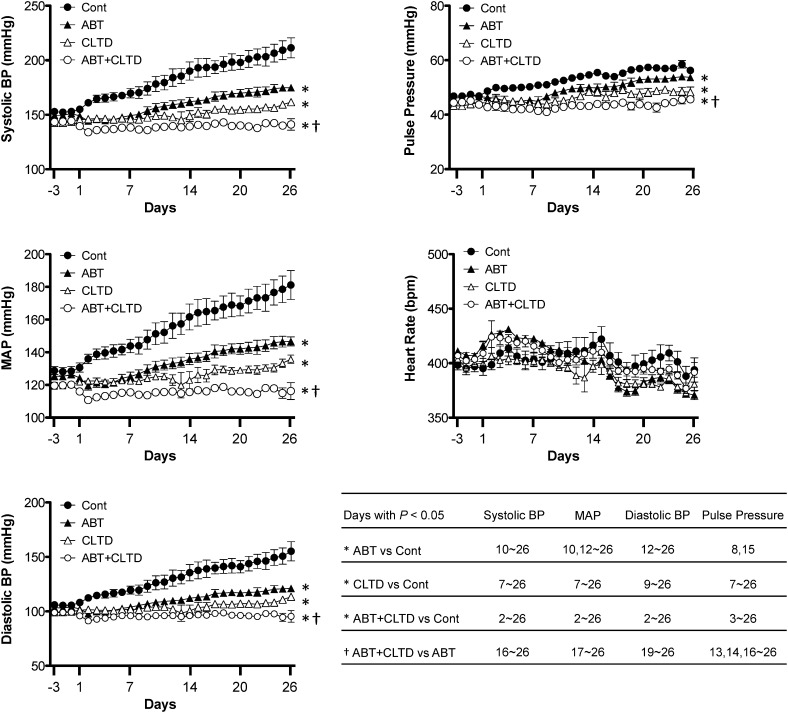
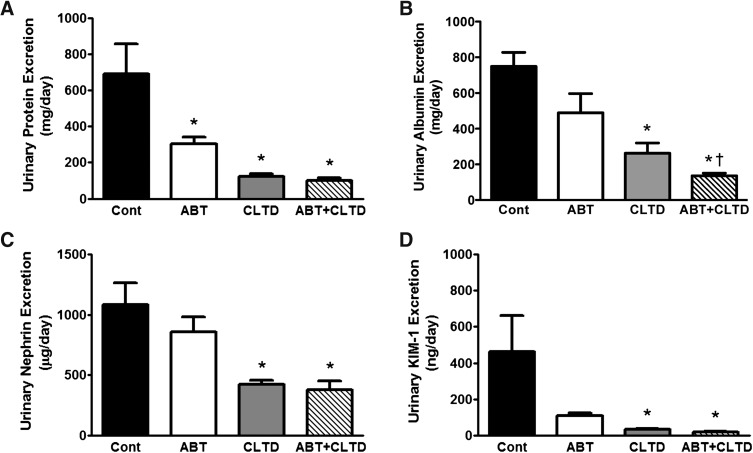
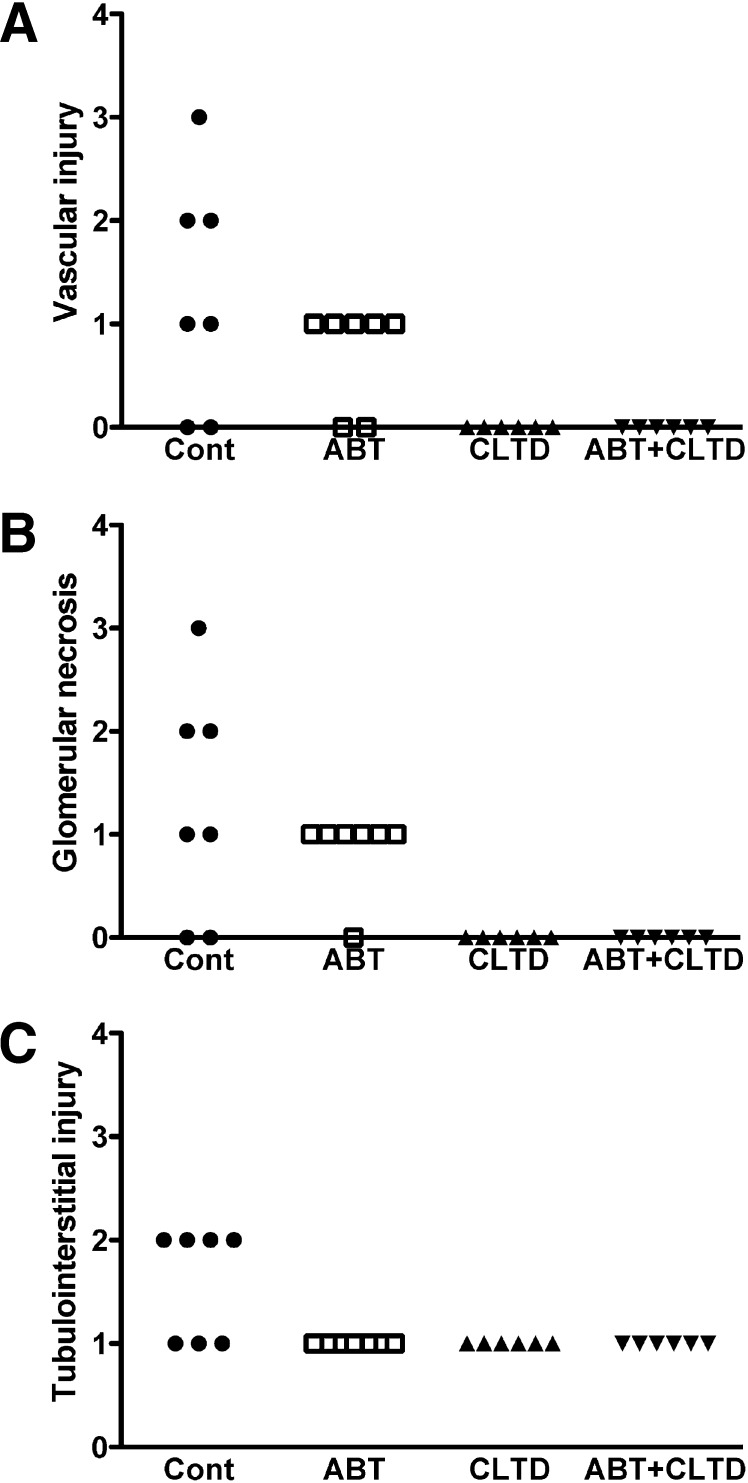
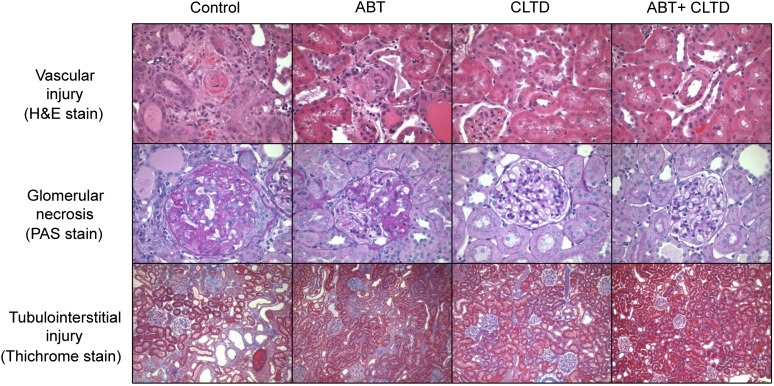
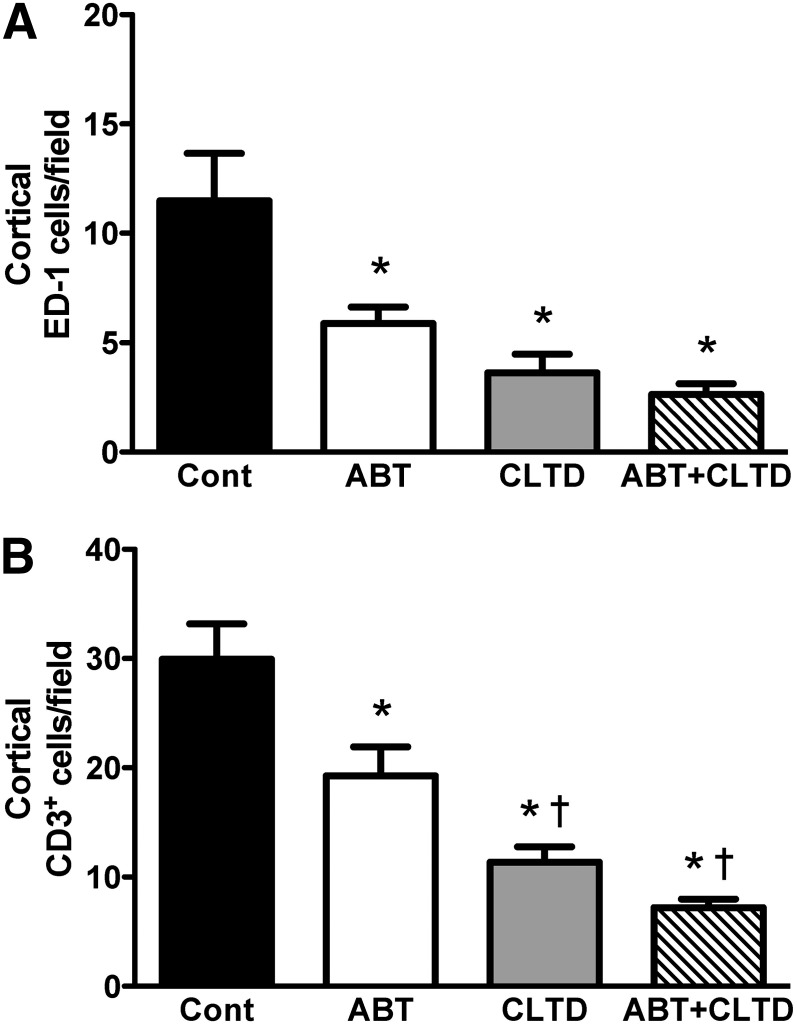
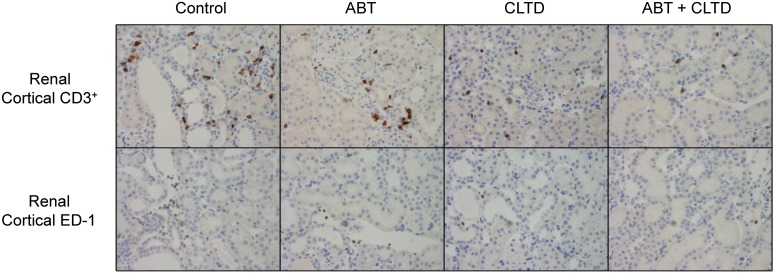
Experiments determined whether the combination of endothelin A (ETA) receptor antagonist [ABT-627, atrasentan; (2R,3R,4S)-4-(1,3-benzodioxol-5-yl)-1-[2-(dibutylamino)-2-oxoethyl]-2-(4-methoxyphenyl)pyrrolidine-3-carboxylic acid] and a thiazide diuretic (chlorthalidone) would be more effective at lowering blood pressure and reducing renal injury in a rodent model of metabolic syndrome compared with either treatment alone. Male Dahl salt-sensitive rats were fed a high-fat (36% fat), high-salt (4% NaCl) diet for 4 weeks. Separate groups of rats were then treated with vehicle (control), ABT-627 (ABT; 5 mg/kg per day, in drinking water), chlorthalidone (CLTD; 5 mg/kg per day, in drinking water), or both ABT plus CLTD. Mean arterial pressure (MAP) was recorded continuously by telemetry. After 4 weeks, both ABT and CLTD severely attenuated the development of hypertension, whereas the combination further reduced MAP compared with ABT alone. All treatments prevented proteinuria. CLTD and ABT plus CLTD significantly reduced nephrin (a podocyte injury marker) and kidney injury molecule-1 (a tubulointerstitial injury marker) excretion. ABT, with or without CLTD, significantly reduced plasma 8-oxo-2'-deoxyguanosine, a measure of DNA oxidation, whereas CLTD alone had no effect. All treatments suppressed the number of ED1(+) cells (macrophages) in the kidney. Plasma tumor necrosis factor receptors 1 and 2 were reduced only in the combined ABT and CLTD group. These results suggest that ABT and CLTD have antihypertensive and renal-protective effects in a model of metabolic syndrome that are maximally effective when both drugs are administered together. The findings support the hypothesis that combined ETA antagonist and diuretic treatment may provide therapeutic benefit for individuals with metabolic syndrome consuming a Western diet.
Copyright © 2014 by The American Society for Pharmacology and Experimental Therapeutics.
Figures
References
-
- Allcock GH, Venema RC, Pollock DM. (1998) ETA receptor blockade attenuates the hypertension but not renal dysfunction in DOCA-salt rats. Am J Physiol 275:R245–R252 - PubMed
-
- Andress DL, Coll B, Pritchett Y, Brennan J, Molitch M, Kohan DE. (2012) Clinical efficacy of the selective endothelin A receptor antagonist, atrasentan, in patients with diabetes and chronic kidney disease (CKD). Life Sci 91:739–742 - PubMed
-
- Bakris GL, Lindholm LH, Black HR, Krum H, Linas S, Linseman JV, Arterburn S, Sager P, Weber M. (2010) Divergent results using clinic and ambulatory blood pressures: report of a darusentan-resistant hypertension trial. Hypertension 56:824–830 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
