

Immunotherapy advances for glioblastoma
- PMID: 25190673
- PMCID: PMC4201077
- DOI: 10.1093/neuonc/nou212
Immunotherapy advances for glioblastoma
Abstract
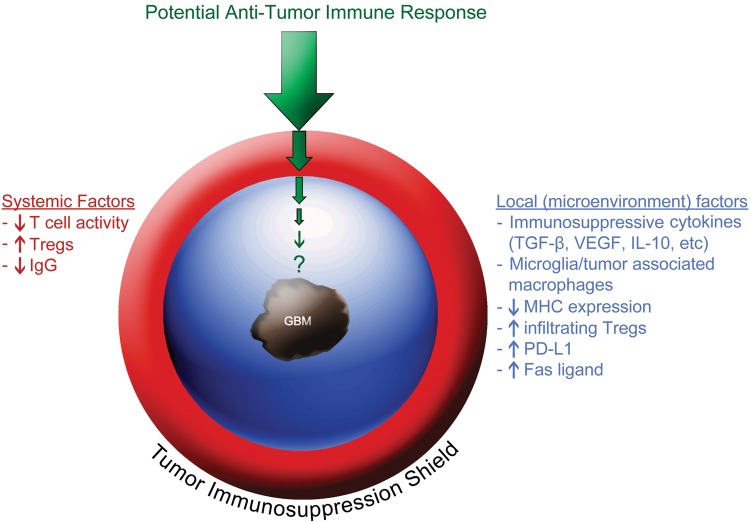
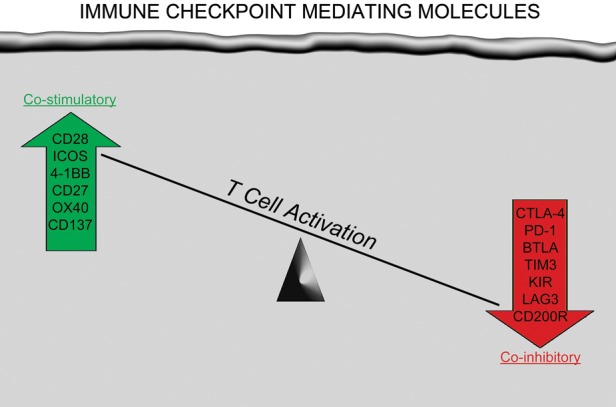
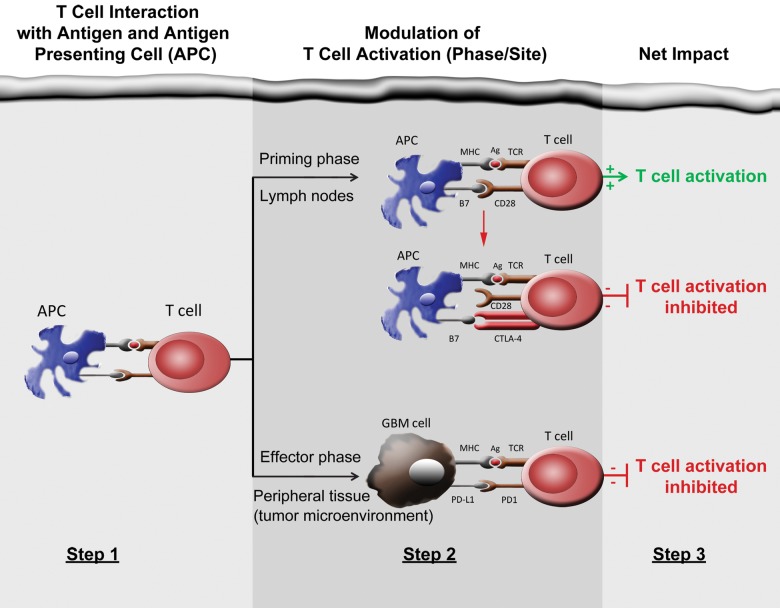
Survival for patients with glioblastoma, the most common high-grade primary CNS tumor, remains poor despite multiple therapeutic interventions including intensifying cytotoxic therapy, targeting dysregulated cell signaling pathways, and blocking angiogenesis. Exciting, durable clinical benefits have recently been demonstrated for a number of other challenging cancers using a variety of immunotherapeutic approaches. Much modern research confirms that the CNS is immunoactive rather than immunoprivileged. Preliminary results of clinical studies demonstrate that varied vaccine strategies have achieved encouraging evidence of clinical benefit for glioblastoma patients, although multiple variables will likely require systematic investigation before optimal outcomes are realized. Initial preclinical studies have also revealed promising results with other immunotherapies including cell-based approaches and immune checkpoint blockade. Clinical studies to evaluate a wide array of immune therapies for malignant glioma patients are being rapidly developed. Important considerations going forward include optimizing response assessment and identifiying correlative biomarkers for predict therapeutic benefit. Finally, the potential of complementary combinatorial immunotherapeutic regimens is highly exciting and warrants expedited investigation.
Keywords: glioblastoma; immune checkpoint; immunosuppression; immunotherapy; vaccine.
© The Author(s) 2014. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Chinot OL, Wick W, Mason W, et al. Bevacizumab plus radiotherapy-temozolomide for newly diagnosed glioblastoma. N Engl J Med. 2014;370(8):709–722. - PubMed
-
- Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. 2010;363(5):411–422. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
