Principles of neuroanesthesia in aneurysmal subarachnoid hemorrhage
- PMID: 25190938
- PMCID: PMC4152670
- DOI: 10.4103/0970-9185.137261
Principles of neuroanesthesia in aneurysmal subarachnoid hemorrhage
Abstract
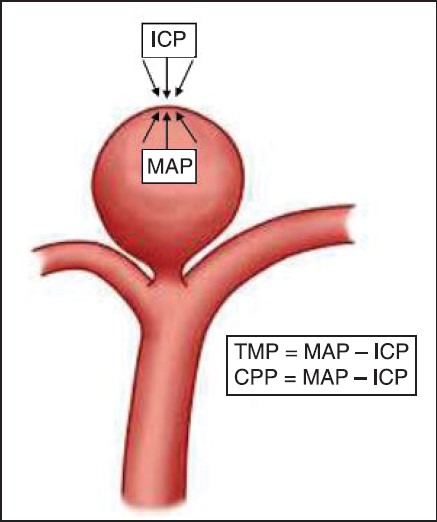
Aneurysmal subarachnoid hemorrhage is associated with high mortality. Understanding of the underlying pathophysiology is important as early intervention can improve outcome. Increasing age, altered sensorium and poor Hunt and Hess grade are independent predictors of adverse outcome. Early operative interventions imposes an onus on anesthesiologists to provide brain relaxation. Coiling and clipping are the two treatment options with increasing trends toward coiling. Intraoperatively, tight control of blood pressure and adequate brain relaxation is desirable, so that accidental aneurysm rupture can be averted. Patients with poor grades tolerate higher blood pressures, but are prone to ischemia whereas patients with lower grades tolerate lower blood pressure, but are prone to aneurysm rupture if blood pressure increases. Patients with Hunt and Hess Grade I or II with uneventful intraoperative course are extubated in operation theater, whereas, higher grades are kept electively ventilated. Postoperative management includes attention toward fluid status and early management of vasospasm.
Keywords: Aneurysm; neuroanesthesia; sub-arachnoid hemorrhage.
Conflict of interest statement
Figures
References
-
- Pong RP, Lam AM. Anaesthetic management of cerebral aneurysm surgery. In: Cotrell JE, Young WL, editors. Neuroanaesthesia. 5th ed. Missouri: Mosby Elsevier; 2010. pp. 218–46.
-
- Macmillan CS, Grant IS, Andrews PJ. Pulmonary and cardiac sequelae of subarachnoid haemorrhage: Time for active management? Intensive Care Med. 2002;28:1012–23. - PubMed
-
- Passier PE, Visser-Meily JM, van Zandvoort MJ, Post MW, Rinkel GJ, van Heugten C. Prevalence and determinants of cognitive complaints after aneurysmal subarachnoid hemorrhage. Cerebrovasc Dis. 2010;29:557–63. - PubMed
-
- de Gans K, Nieuwkamp DJ, Rinkel GJ, Algra A. Timing of aneurysm surgery in subarachnoid hemorrhage: A systematic review of the literature. Neurosurgery. 2002;50:336–40. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical