Analgesic efficacy of transversus abdominis plane block in providing effective perioperative analgesia in patients undergoing total abdominal hysterectomy: A randomized controlled trial
- PMID: 25190950
- PMCID: PMC4152682
- DOI: 10.4103/0970-9185.137274
Analgesic efficacy of transversus abdominis plane block in providing effective perioperative analgesia in patients undergoing total abdominal hysterectomy: A randomized controlled trial
Abstract
Background and aims: Transversus abdominis plane (TAP) block has been shown to provide postoperative pain relief following various abdominal and inguinal surgeries, but few studies have evaluated its analgesic efficacy for intraoperative analgesia. We evaluated the efficacy of TAP block in providing effective perioperative analgesia in total abdominal hysterectomy in a randomized double-blind controlled clinical trial.
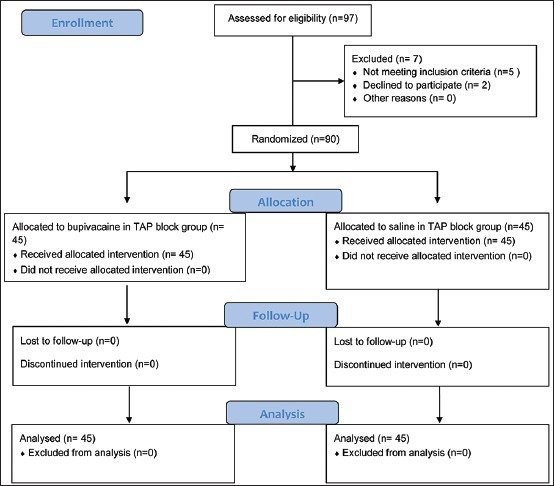
Materials and methods: A total of 90 adult female patients American Society of Anesthesiologists physical status I or II were randomized to Group B (n = 45) receiving TAP block with 0.25% bupivacaine and Group N (n = 45) with normal saline followed by general anesthesia. Hemodynamic responses to surgical incision and intraoperative fentanyl consumption were noted. Visual analog scale (VAS) scores were assessed on the emergence, at 1, 2, 3, 4, 5, 6 and 24 h. Time to first rescue analgesic (when VAS ≥4 cm or on demand), duration of postoperative analgesia, incidence of postoperative nausea-vomiting were also noted.
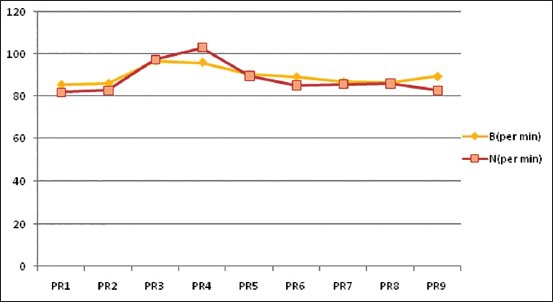
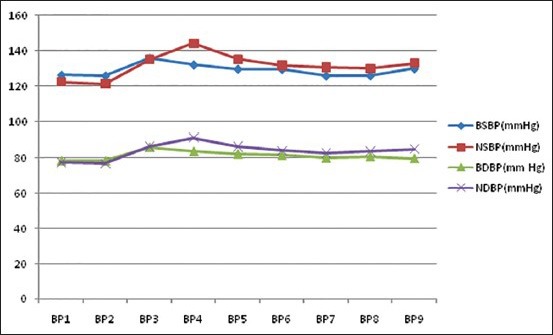
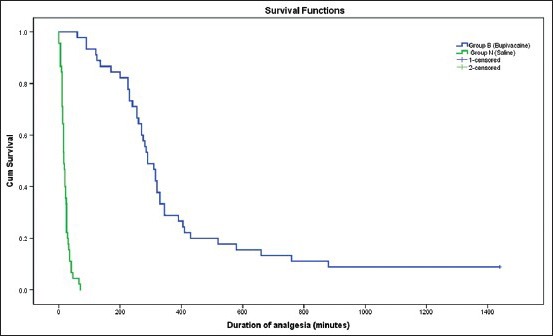
Results: Pulse rate (95.9 ± 11.2 bpm vs. 102.9 ± 8.8 bpm, P = 0.001) systolic and diastolic BP were significantly higher in Group N. Median intraoperative fentanyl requirement was significantly higher in Group N (81 mcg vs. 114 mcg, P = 0.000). VAS scores on emergence at rest (median VAS 3 mm vs 27 mm), with activity (median 8 mm vs. 35 mm) were significantly lower in Group B. Median duration of analgesia was significantly higher in Group B (290 min vs. 16 min, P = 0.000). No complication or opioid related side effect attributed to TAP block were noted in any patient.
Conclusion: Preincisional TAP block decreases intraoperative fentanyl requirements, prevents hemodynamic responses to surgical stimuli and provides effective postoperative analgesia.
Keywords: Abdominal hysterectomy; perioperative analgesia; transversus abdominis plane block.
Conflict of interest statement
Figures
References
-
- Rafi AN. Abdominal field block: A new approach via the lumbar triangle. Anaesthesia. 2001;56:1024–6. - PubMed
-
- McDonnell JG, O’Donnell B, Curley G, Heffernan A, Power C, Laffey JG. The analgesic efficacy of transversus abdominis plane block after abdominal surgery: A prospective randomized controlled trial. Anesth Analg. 2007;104:193–7. - PubMed
-
- Carney J, Finnerty O, Rauf J, Curley G, McDonnell JG, Laffey JG. Ipsilateral transversus abdominis plane block provides effective analgesia after appendectomy in children: A randomized controlled trial. Anesth Analg. 2010;111:998–1003. - PubMed
-
- O’Donnell BD, McDonnell JG, McShane AJ. The transversus abdominis plane (TAP) block in open retropubic prostatectomy. Reg Anesth Pain Med. 2006;31:91. - PubMed
-
- Hosgood SA, Thiyagarajan UM, Nicholson HF, Jeyapalan I, Nicholson ML. Randomized clinical trial of transversus abdominis plane block versus placebo control in live-donor nephrectomy. Transplantation. 2012;94:520–5. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous