

Current practice and recommendation for presurgical cardiac evaluation in patients undergoing noncardiac surgeries
- PMID: 25191106
- PMCID: PMC4149772
- DOI: 10.4103/1450-1147.138568
Current practice and recommendation for presurgical cardiac evaluation in patients undergoing noncardiac surgeries
Abstract
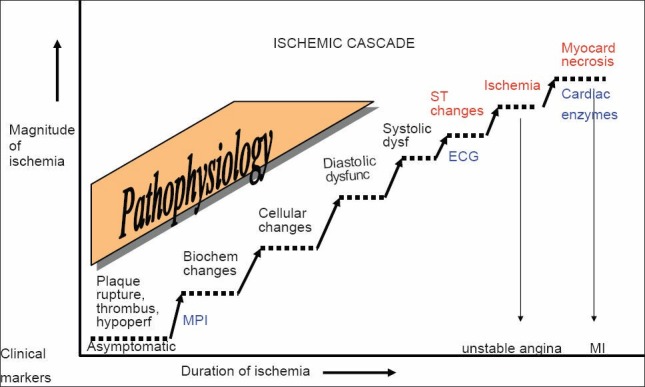
The increasing number of patients with coronary artery disease (CAD) undergoing major noncardiac surgery justifies guidelines concerning preoperative cardiac evaluation. This is compounded by increasing chances for a volatile perioperative period if the underlying cardiac problems are left uncorrected prior to major noncardiac surgeries. Preoperative cardiac evaluation requires the clinician to assess the patient's probability to have CAD, severity and stability of CAD, placing these in perspective regarding the likelihood of a perioperative cardiac complication based on the planned surgical procedure. Coronary events like new onset ischemia, infarction, or revascularization, induce a high-risk period of 6 weeks, and an intermediate-risk period of 3 months before performing noncardiac surgery. This delay is unwarranted in cases where surgery is the mainstay of treatment. The objective of this review is to offer a comprehensive algorithm in the preoperative assessment of patients undergoing noncardiac surgery and highlight the importance of myocardial perfusion imaging in risk stratifying these patients.
Keywords: Cardiac risk stratification; coronary artery disease; heart; noncardiac surgeries; stress myocardial perfusion imaging; surgery.
Conflict of interest statement
Figures
References
-
- Maddox TM. Preoperative cardiovascular evaluation for noncardiac surgery. Mt Sinai J Med. 2005;72:185–92. - PubMed
-
- Rao TL, Jacobs KH, El-Etr AA. Reinfarction following anesthesia in patients with myocardial infarction. Anesthesiology. 1983;59:499–505. - PubMed
-
- Chassot PG, Delabays A, Spahn DR. Preoperative evaluation of patients with, or at risk of, coronary artery disease undergoing non-cardiac surgery. Br J Anaesth. 2002;89:747–59. - PubMed
-
- Ashton CM, Petersen NJ, Wray NP, Kiefe CI, Dunn JK, Wu L, et al. The incidence of perioperative myocardial infarction in men undergoing noncardiac surgery. Ann Intern Med. 1993;118:504–10. - PubMed
-
- Patel AD, Abo-Auda WS, Davis JM, Zoghbi GJ, Deierhoi MH, Heo J, et al. Prognostic value of myocardial perfusion imaging in predicting outcome after renal transplantation. Am J Cardiol. 2003;92:146–51. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous