

Enhanced upper-airway muscle responsiveness is a distinct feature of overweight/obese individuals without sleep apnea
- PMID: 25191791
- PMCID: PMC4299579
- DOI: 10.1164/rccm.201404-0783OC
Enhanced upper-airway muscle responsiveness is a distinct feature of overweight/obese individuals without sleep apnea
Abstract
Rationale: Body habitus is a major determinant of obstructive sleep apnea (OSA). However, many individuals do not have OSA despite being overweight/obese (body mass index > 25 kg/m(2)) for reasons that are not fully elucidated.
Objectives: To determine the key physiologic traits (upper-airway anatomy/collapsibility, upper-airway muscle responsiveness, chemoreflex control of ventilation, arousability from sleep) responsible for the absence of OSA in overweight/obese individuals.
Methods: We compared key physiologic traits in 18 overweight/obese subjects without apnea (apnea-hypopnea index < 15 events per hour) with 25 overweight/obese matched patients with OSA (apnea-hypopnea index ≥ 15 events per hour) and 11 normal-weight nonapneic control subjects. Traits were measured by repeatedly lowering continuous positive airway pressure to subtherapeutic levels for 3 minutes during non-REM sleep.
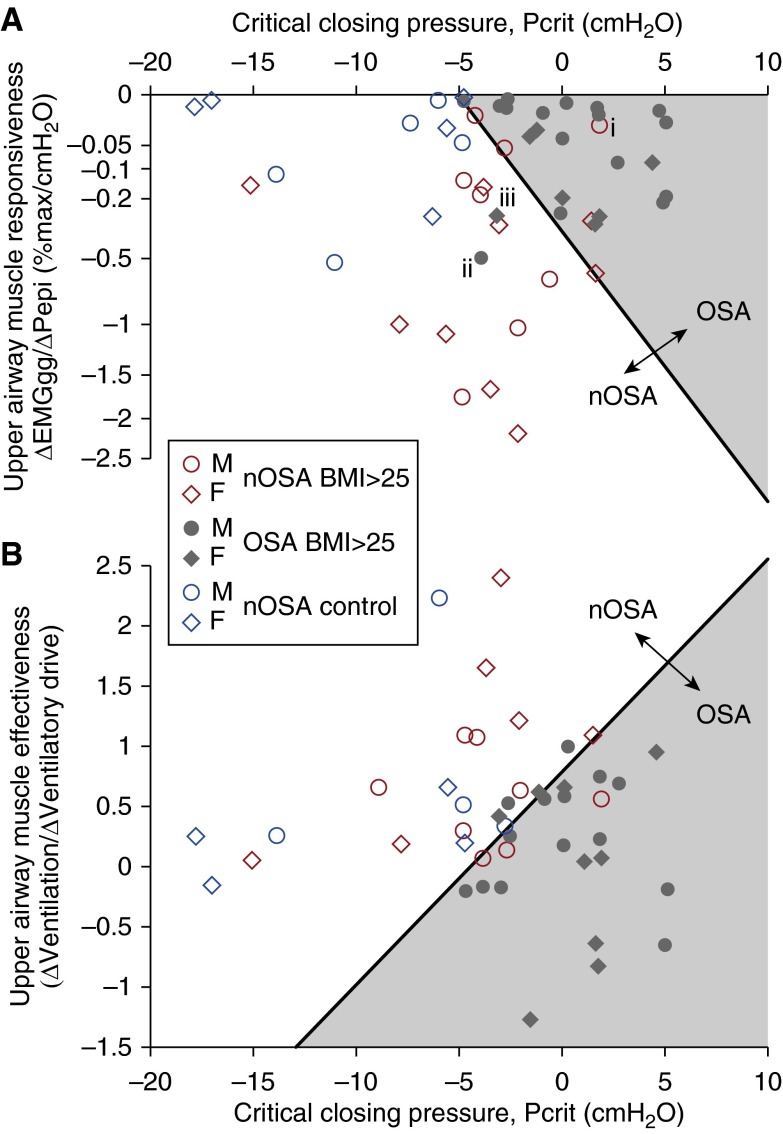
Measurements and main results: Overweight/obese subjects without apnea exhibited a less collapsible airway than overweight/obese patients with apnea (critical closing pressure: -3.7 ± 1.9 vs. 0.6 ± 1.2 cm H2O; P = 0.003; mean ± 95% confidence interval), but a more collapsible airway relative to normal-weight control subjects (-8.8 ± 3.1 cm H2O; P < 0.001). Notably, overweight/obese subjects without apnea exhibited a threefold greater upper-airway muscle responsiveness than both overweight/obese patients with apnea (Δgenioglossus EMG/Δepiglottic pressure: -0.49 [-0.22 to -0.79] vs. -0.15 [-0.09 to -0.22] %max/cm H2O; P = 0.008; mean [95% confidence interval]) and normal-weight control subjects (-0.16 [-0.04 to -0.30] %max/cm H2O; P = 0.02). Loop gain was elevated (more negative) in both overweight/obese groups and normal-weight control subjects (P = 0.02). Model-based analysis demonstrated that overweight/obese individuals without apnea rely on both more favorable anatomy and collapsibility and enhanced upper-airway dilator muscle responses to avoid OSA.
Conclusions: Overweight/obese individuals without apnea have a moderately compromised upper-airway structure that is mitigated by highly responsive upper-airway dilator muscles to avoid OSA. Elucidating the mechanisms underlying enhanced muscle responses in this population may provide clues for novel OSA interventions.
Keywords: apnea phenotypes; control of breathing; mathematical model; obesity; upper airway muscles.
Figures




Comment in
-
Obesity-related ventilatory phenotypes of sleep-disordered breathing.Am J Respir Crit Care Med. 2014 Oct 15;190(8):853-4. doi: 10.1164/rccm.201409-1674ED. Am J Respir Crit Care Med. 2014. PMID: 25317463 No abstract available.
References
-
- Pahkala R, Seppa J, Ikonen A, Smirnov G, Tuomilehto H. The impact of pharyngeal fat tissue on the pathogenesis of obstructive sleep apnea. Sleep Breath. 2014;18:275–282. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
