

Reliability and clinical test performance of cochlear reflectance
- PMID: 25192133
- PMCID: PMC4272609
- DOI: 10.1097/AUD.0000000000000089
Reliability and clinical test performance of cochlear reflectance
Abstract
Objective: Cochlear reflectance (CR) is the cochlear contribution to ear-canal reflectance. CR is equivalent to an otoacoustic emission (OAE) deconvolved by forward pressure in the ear canal. Similar to other OAE measures, CR level is related to cochlear status. When measured using wideband noise stimuli, potential advantages of CR over other types of OAEs include (1) the capability to cover a wider frequency range more efficiently by requiring fewer measurements, (2) minimal influence on the recorded emission from the measurement system and middle ear, (3) lack of entrainment of spontaneous OAEs, and (4) easier interpretation because of the existence of an equivalent linear model, which validates the application of linear systems theory. The purposes of this study were to evaluate the reliability, assess the accuracy in a clinical screening paradigm, and determine the relation of CR to audiometric thresholds. Thus, this study represents an initial assessment of the clinical utility of CR.
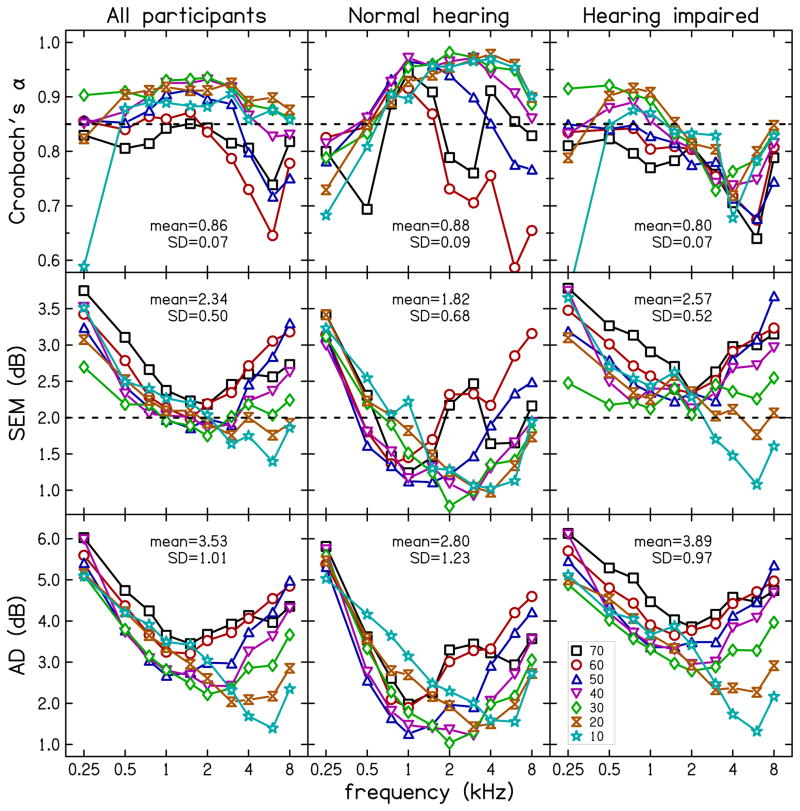
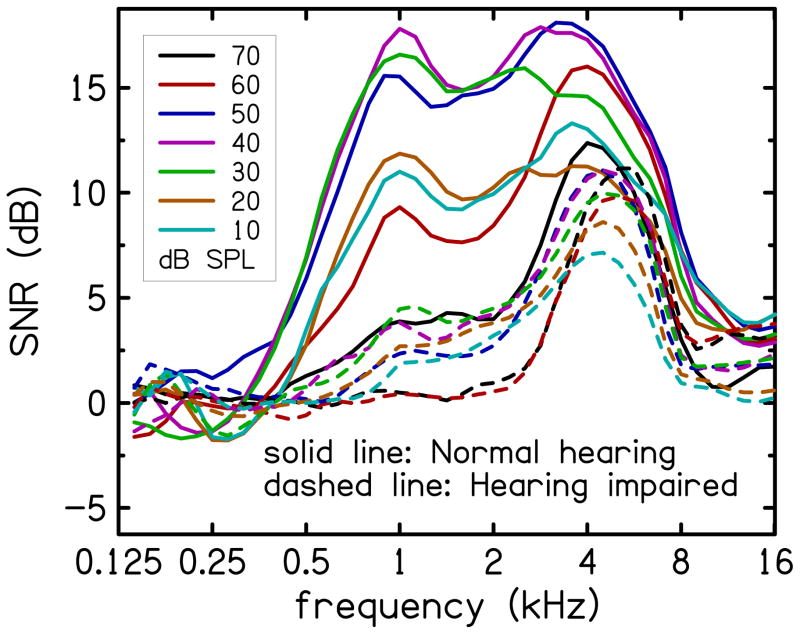
Design: Data were collected from 32 normal-hearing and 58 hearing-impaired participants. A wideband noise stimulus presented at seven stimulus levels (10 to 70 dB SPL, 10 dB steps) was used to elicit the CR. Reliability of CR was assessed using Cronbach's α, standard error of measurement, and absolute differences between CR data from three separate test sessions. Test performance was evaluated using clinical decision theory. The ability of CR to predict audiometric thresholds was evaluated using regression analysis.
Results: CR repeatability across test sessions was similar to that of other clinical measurements. However, both the accuracy with which CR distinguished normal-hearing from hearing-impaired ears and the accuracy with which CR predicted audiometric thresholds were less than those reported in previous studies using distortion-product OAE measurements.
Conclusions: CR measurements are repeatable between test sessions, can be used to predict auditory status, and are related to audiometric thresholds. However, under current conditions, CR does not perform as well as other OAE measurements. Further developments in CR measurement and analysis methods may improve performance. CR has theoretical advantages for cochlear modeling, which may lead to improved interpretation of cochlear status.
Figures









References
-
- Allen JB. Measurement of eardrum acoustic impedance. In: Allen JB, Hall JL, Hubbard A, Neely ST, Tubis A, editors. Peripheral Auditory Mechanisms. Springer-Verlag; New York: 1986.
-
- Allen JB. Derecruitment by multiband compression in hearing aids. In: Jesteadt W, editor. Modeling Sensorineural hearing loss. Lawrence Erlbaum Associates; New Jersey: 1997. pp. 99–112.
-
- Boege P, Janssen T. Pure-tone threshold estimation from extrapolated distortion product otoacoustic emissions I/O-functions in normal and cochlear hearing loss ears. J Acoust Soc Am. 2002;111:1810–1818. - PubMed
-
- Cronbach LJ. Coefficient alpha and the internal structure of tests. Psychometrika. 1951;16:297–334.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
