

New diagnosis and therapy model for ischemic-type biliary lesions following liver transplantation--a retrospective cohort study
- PMID: 25192214
- PMCID: PMC4156319
- DOI: 10.1371/journal.pone.0105795
New diagnosis and therapy model for ischemic-type biliary lesions following liver transplantation--a retrospective cohort study
Retraction in
-
Retraction: New Diagnosis and Therapy Model for Ischemic-Type Biliary Lesions following Liver Transplantation-A Retrospective Cohort Study.PLoS One. 2019 Sep 6;14(9):e0222409. doi: 10.1371/journal.pone.0222409. eCollection 2019. PLoS One. 2019. PMID: 31491018 Free PMC article. No abstract available.
Abstract
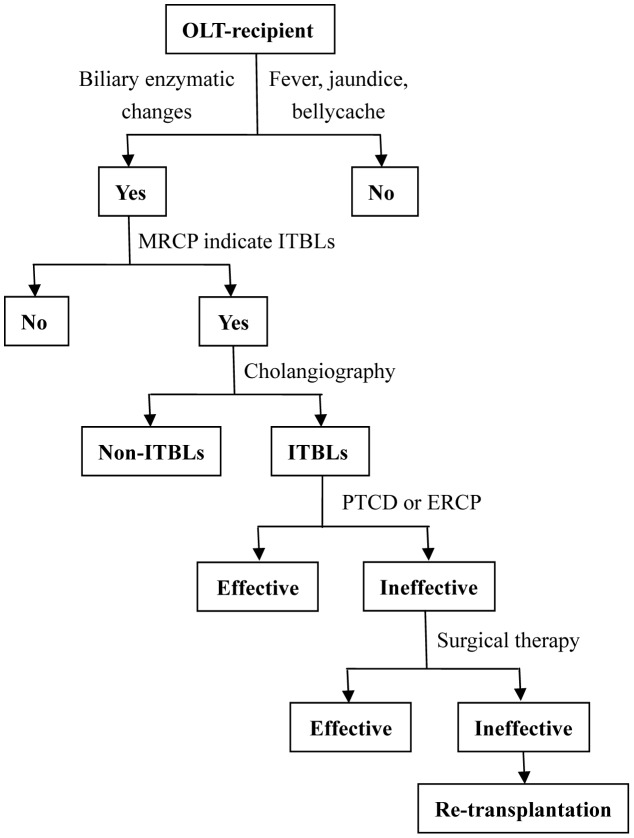
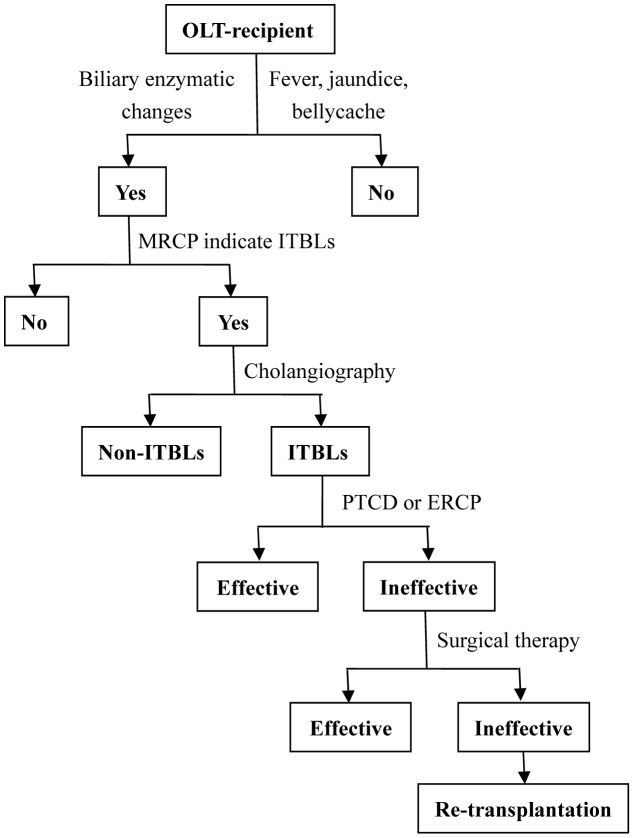
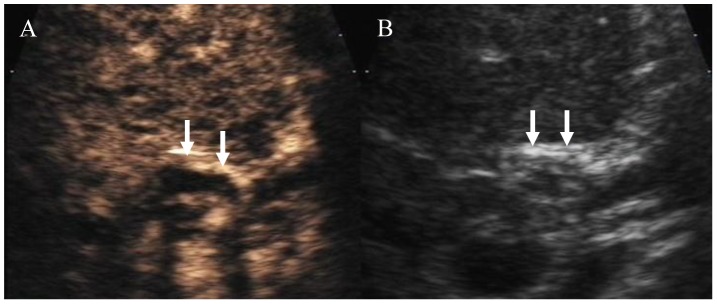
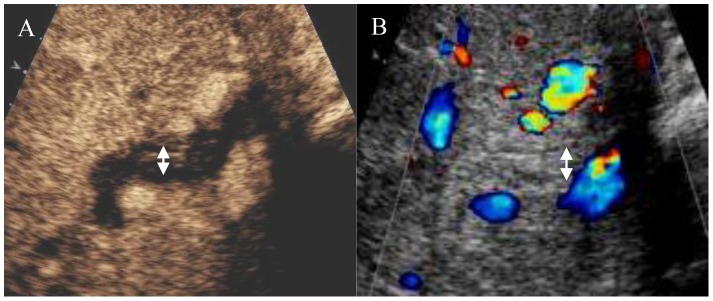
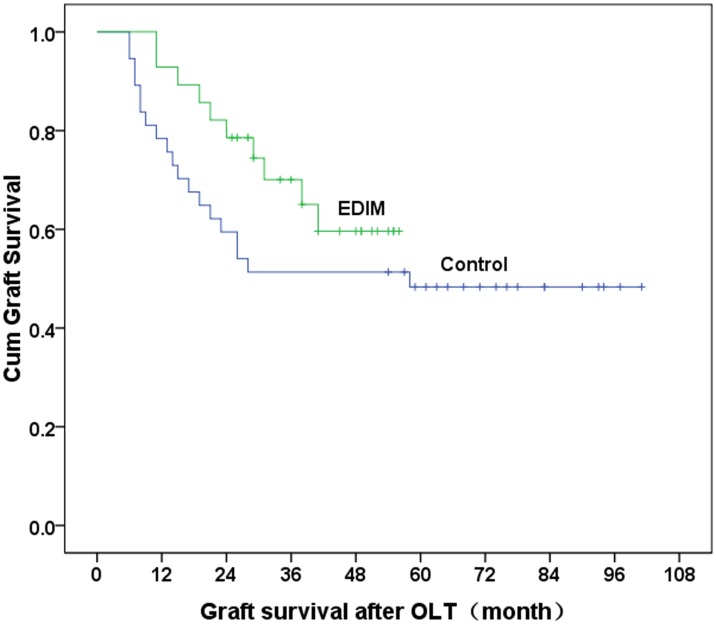
Ischemic-type biliary lesions (ITBLs) are a major cause of graft loss and mortality after orthotopic liver transplantation (OLT). Impaired blood supply to the bile ducts may cause focal or extensive damage, resulting in intra- or extrahepatic bile duct strictures or dilatations that can be detected by ultrasonography, computed tomography, magnetic resonance cholangiopancreatography, and cholangiography. However, the radiographic changes occur at an advanced stage, after the optimal period for therapeutic intervention. Endoscopic retrograde cholangio-pancreatography (ERCP) and percutaneous transhepatic cholangiodrainage (PTCD) are the gold standard methods of detecting ITBLs, but these procedures cannot be used for continuous monitoring. Traditional methods of follow-up and diagnosis result in delayed diagnosis and treatment of ITBLs. Our center has used the early diagnosis and intervention model (EDIM) for the diagnosis and treatment of ITBLs since February 2008. This model mainly involves preventive medication to protect the epithelial cellular membrane of the bile ducts, regular testing of liver function, and weekly monitor of contrast-enhanced ultrasonography (CEUS) to detect ischemic changes to the bile ducts. If the liver enzyme levels become abnormal or CEUS shows low or no enhancement of the wall of the hilar bile duct during the arterial phase, early ERCP and PTCD are performed to confirm the diagnosis and to maintain biliary drainage. Compared with patients treated by the traditional model used prior to February 2008, patients in the EDIM group had a lower incidence of biliary tract infection (28.6% vs. 48.6%, P = 0.04), longer survival time of liver grafts (24±9.6 months vs. 17±12.3 months, P = 0.02), and better outcomes after treatment of ITBLs.
Conflict of interest statement
Figures
Similar articles
-
Revealing impaired blood supply to the bile ducts on contrast-enhanced ultrasound: a novel diagnosis method to ischemic-type biliary lesions after orthotropic liver transplantation.Ultrasound Med Biol. 2013 May;39(5):753-60. doi: 10.1016/j.ultrasmedbio.2012.12.004. Epub 2013 Mar 7. Ultrasound Med Biol. 2013. PMID: 23465141 Clinical Trial.
-
Optimized endoscopic treatment of ischemic-type biliary lesions after liver transplantation.Gastrointest Endosc. 2012 Sep;76(3):556-63. doi: 10.1016/j.gie.2012.04.474. Gastrointest Endosc. 2012. PMID: 22898414
-
An endoscopic approach to biliary complications following orthotopic liver transplantation.Liver Int. 2003 Jun;23(3):156-62. doi: 10.1034/j.1600-0676.2003.00823.x. Liver Int. 2003. PMID: 12955878
-
Causes and consequences of ischemic-type biliary lesions after liver transplantation.J Hepatobiliary Pancreat Surg. 2006;13(6):517-24. doi: 10.1007/s00534-005-1080-2. Epub 2006 Nov 30. J Hepatobiliary Pancreat Surg. 2006. PMID: 17139425 Review.
-
Bile duct complications after liver transplantation.Transpl Int. 2005 Jun;18(6):627-42. doi: 10.1111/j.1432-2277.2005.00123.x. Transpl Int. 2005. PMID: 15910286 Review.
Cited by
-
Initial study of sediment antagonism and characteristics of silver nanoparticle-coated biliary stents in an experimental animal model.Int J Nanomedicine. 2016 Apr 28;11:1807-17. doi: 10.2147/IJN.S103609. eCollection 2016. Int J Nanomedicine. 2016. PMID: 27217749 Free PMC article.
-
Application of contrast-enhanced ultrasound after liver transplantation: Current status and perspectives.World J Gastroenterol. 2016 Jan 28;22(4):1607-16. doi: 10.3748/wjg.v22.i4.1607. World J Gastroenterol. 2016. PMID: 26819526 Free PMC article. Review.
-
Secondary sclerosing cholangitis and IgG4-sclerosing cholangitis - A review of cholangiographic and ultrasound imaging.Endosc Ultrasound. 2023 Mar-Apr;12(2):181-199. doi: 10.4103/EUS-D-22-00208. Endosc Ultrasound. 2023. PMID: 36588352 Free PMC article. Review.
-
Evaluation value of contrast enhanced ultrasound quantitative parameters in ischemic-type biliary lesions after liver transplantation-a prospectively study.Abdom Radiol (NY). 2025 Aug;50(8):3497-3505. doi: 10.1007/s00261-024-04761-3. Epub 2025 Jan 25. Abdom Radiol (NY). 2025. PMID: 39862289
-
Retraction: New Diagnosis and Therapy Model for Ischemic-Type Biliary Lesions following Liver Transplantation-A Retrospective Cohort Study.PLoS One. 2019 Sep 6;14(9):e0222409. doi: 10.1371/journal.pone.0222409. eCollection 2019. PLoS One. 2019. PMID: 31491018 Free PMC article. No abstract available.
References
-
- Buis CI, Hoekstra H, Verdonk RC, Porte RJ (2006) Causes and consequences of ischemic-type biliary lesions after liver transplantation. J Hepatobiliary Pancreat Surg 13: 517–524. - PubMed
-
- Sawyer RG, Punch JD (1998) Incidence and management of biliary complications after 291 liver transplants following the introduction of transcystic stenting. Transplantation 66: 1201–1207. - PubMed
-
- Turrion VS, Alvira LG, Jimenez M, Lucena JL, Nuno J, et al. (1999) Management of the biliary complications associated with liver transplantation: 13 years of experience. Transplant Proc 31: 2392–2393. - PubMed
-
- Rizk RS, McVicar JP, Emond MJ, Rohrmann CA Jr, Kowdley KV, et al. (1998) Endoscopic management of biliary strictures in liver transplant recipients: effect on patient and graft survival. Gastrointest Endosc 47: 128–135. - PubMed
-
- Ward EM, Kiely MJ, Maus TP, Wiesner RH, Krom RA (1990) Hilar biliary strictures after liver transplantation: cholangiography and percutaneous treatment. Radiology 177: 259–263. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
