

Evaluation and management of patients with heart disease and cancer: cardio-oncology
- PMID: 25192616
- PMCID: PMC4258909
- DOI: 10.1016/j.mayocp.2014.05.013
Evaluation and management of patients with heart disease and cancer: cardio-oncology
Abstract
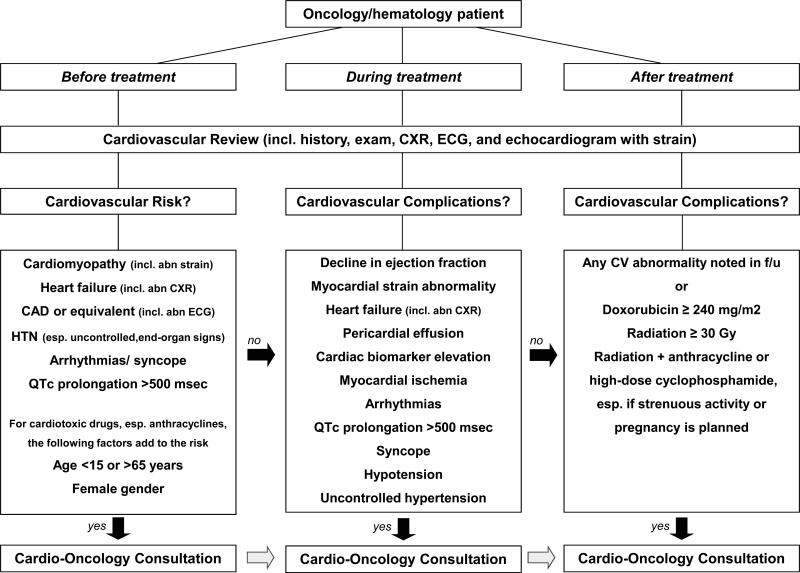
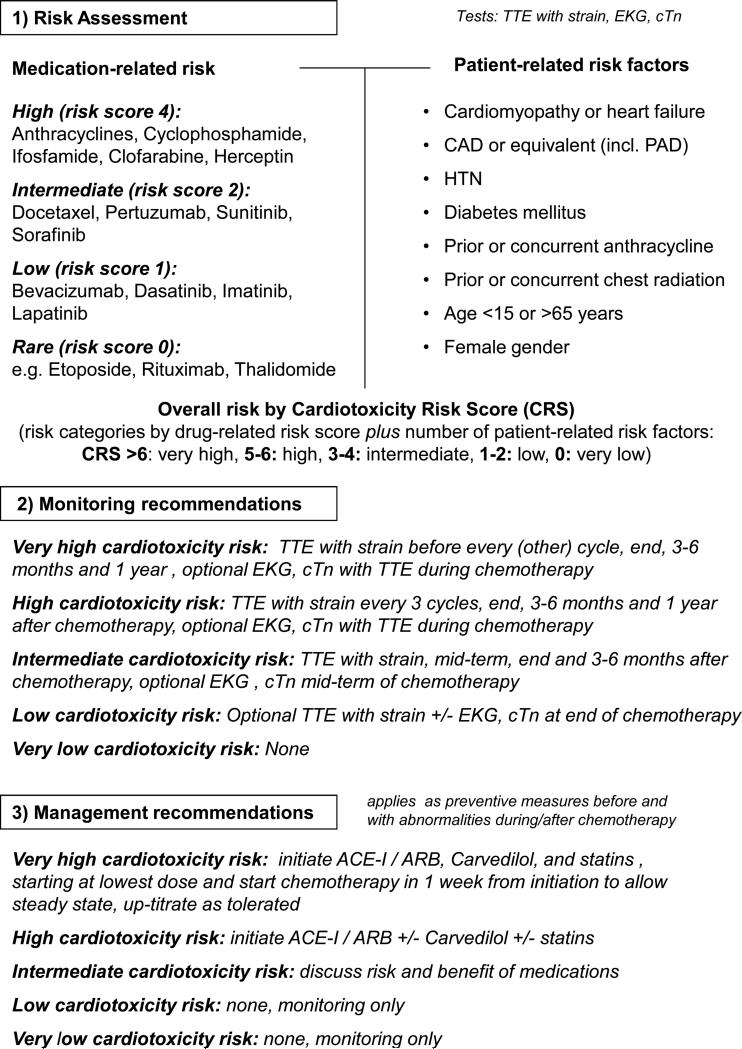
The care for patients with cancer has advanced greatly over the past decades. A combination of earlier cancer diagnosis and greater use of traditional and new systemic treatments has decreased cancer-related mortality. Effective cancer therapies, however, can result in short- and long-term comorbidities that can decrease the net clinical gain by affecting quality of life and survival. In particular, cardiovascular complications of cancer treatments can have a profound effect on the health of patients with cancer and are more common among those with recognized or unrecognized underlying cardiovascular diseases. A new discipline termed cardio-oncology has thus evolved to address the cardiovascular needs of patients with cancer and optimize their care in a multidisciplinary approach. This review provides a brief introduction and background on this emerging field and then focuses on its practical aspects including cardiovascular risk assessment and prevention before cancer treatment, cardiovascular surveillance and therapy during cancer treatment, and cardiovascular monitoring and management after cancer therapy. The content of this review is based on a literature search of PubMed between January 1, 1960, and February 1, 2014, using the search terms cancer, cardiomyopathy, cardiotoxicity, cardio-oncology, chemotherapy, heart failure, and radiation.
Copyright © 2014 Mayo Foundation for Medical Education and Research. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Lee CK, Aeppli D, Nierengarten ME. The need for long-term surveillance for patients treated with curative radiotherapy for Hodgkin's disease: University of Minnesota experience. International journal of radiation oncology, biology, physics. 2000;48:169–179. - PubMed
-
- Jaworski C, Mariani JA, Wheeler G, Kaye DM. Cardiac complications of thoracic irradiation. Journal of the American College of Cardiology. 2013 - PubMed
-
- Aapro M, Bernard-Marty C, Brain EG, et al. Anthracycline cardiotoxicity in the elderly cancer patient: a SIOG expert position paper. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO. 2011;22:257–267. - PubMed
-
- Serrano C, Cortes J, De Mattos-Arruda L, et al. Trastuzumab-related cardiotoxicity in the elderly: a role for cardiovascular risk factors. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO. 2012;23:897–902. - PubMed
-
- Tarantini L, Gori S, Faggiano P, et al. Adjuvant trastuzumab cardiotoxicity in patients over 60 years of age with early breast cancer: a multicenter cohort analysis. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO. 2012;23:3058–3063. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
