

Population-based screening for breast and ovarian cancer risk due to BRCA1 and BRCA2
- PMID: 25192939
- PMCID: PMC4191771
- DOI: 10.1073/pnas.1415979111
Population-based screening for breast and ovarian cancer risk due to BRCA1 and BRCA2
Abstract
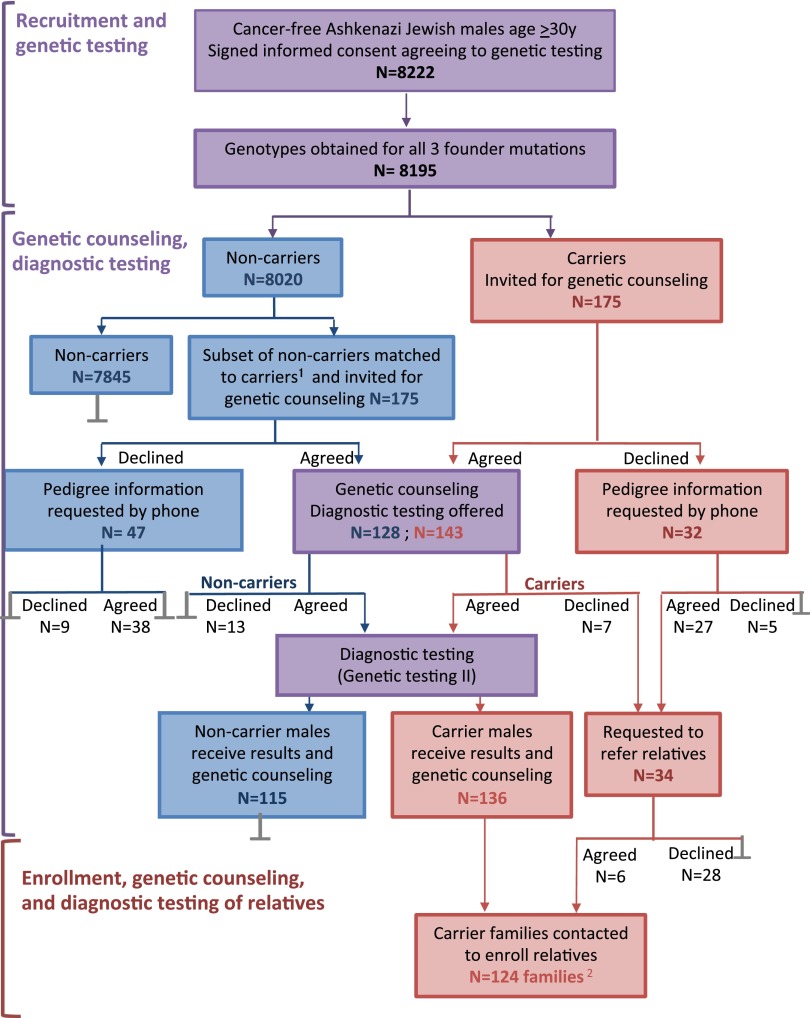
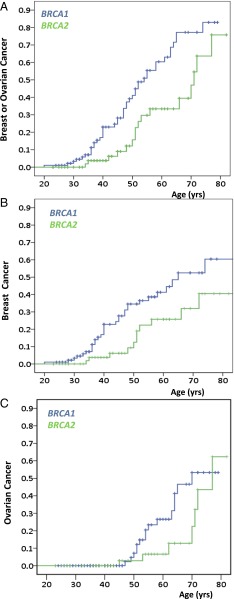
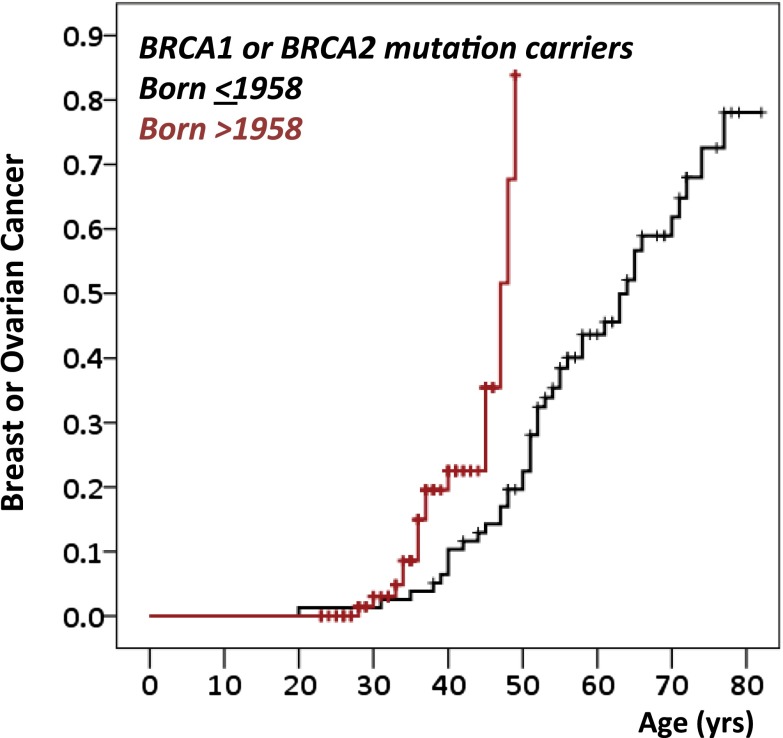
In the Ashkenazi Jewish (AJ) population of Israel, 11% of breast cancer and 40% of ovarian cancer are due to three inherited founder mutations in the cancer predisposition genes BRCA1 and BRCA2. For carriers of these mutations, risk-reducing salpingo-oophorectomy significantly reduces morbidity and mortality. Population screening for these mutations among AJ women may be justifiable if accurate estimates of cancer risk for mutation carriers can be obtained. We therefore undertook to determine risks of breast and ovarian cancer for BRCA1 and BRCA2 mutation carriers ascertained irrespective of personal or family history of cancer. Families harboring mutations in BRCA1 or BRCA2 were ascertained by identifying mutation carriers among healthy AJ males recruited from health screening centers and outpatient clinics. Female relatives of the carriers were then enrolled and genotyped. Among the female relatives with BRCA1 or BRCA2 mutations, cumulative risk of developing either breast or ovarian cancer by age 60 and 80, respectively, were 0.60 (± 0.07) and 0.83 (± 0.07) for BRCA1 carriers and 0.33 (± 0.09) and 0.76 (± 0.13) for BRCA2 carriers. Risks were higher in recent vs. earlier birth cohorts (P = 0.006). High cancer risks in BRCA1 or BRCA2 mutation carriers identified through healthy males provide an evidence base for initiating a general screening program in the AJ population. General screening would identify many carriers who are not evaluated by genetic testing based on family history criteria. Such a program could serve as a model to investigate implementation and outcomes of population screening for genetic predisposition to cancer in other populations.
Keywords: genomics.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- King MC, Marks JH, Mandell JB. New York Breast Cancer Study Group Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science. 2003;302(5645):643–646. - PubMed
-
- Møller P, et al. Genetic epidemiology of BRCA mutations—family history detects less than 50% of the mutation carriers. Eur J Cancer. 2007;43(11):1713–1717. - PubMed
-
- Weitzel JN, et al. Limited family structure and BRCA gene mutation status in single cases of breast cancer. JAMA. 2007;297(23):2587–2595. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
