

Review
doi: 10.1161/JAHA.114.001111.
Insights into aortic sclerosis and its relationship with coronary artery disease
Affiliations
- PMID: 25193296
- PMCID: PMC4323780
- DOI: 10.1161/JAHA.114.001111
Item in Clipboard
Review
Insights into aortic sclerosis and its relationship with coronary artery disease
J Am Heart Assoc.
.
No abstract available
Keywords: Aortic stenosis; aortic valve calcification; atherosclerosis; cardiovascular outcomes; cardiovascular pathophysiology.
Figures
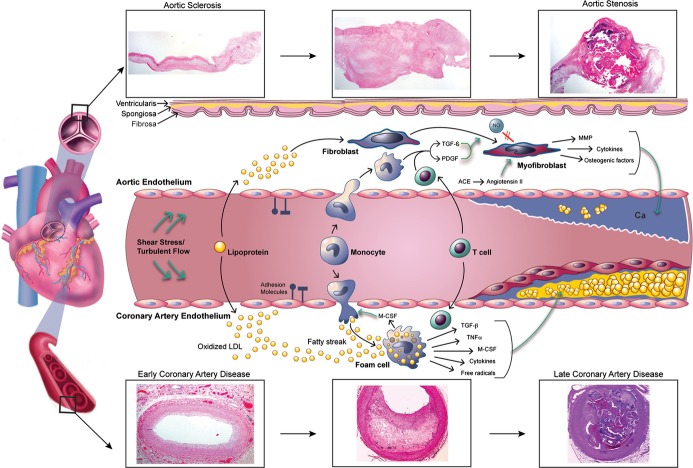
Pathophysiology of aortic sclerosis, aortic stenosis, and coronary artery disease. The evolution from normal vasculature to aortic stenosis and coronary artery disease shares several important cellular mechanisms including lipid deposition, inflammatory cell infiltration, cytokine release, and calcification. While a smooth muscle cap overlying a lipid core develops in coronary artery disease, aortic stenosis is characterized by thick calcifications. Pathology of human aortic valves and coronary arteries illustrates this transition at the tissue level. ACE indicates angiotensin‐converting enzyme; Ca, calcium; LDL, low‐density lipoprotein; M‐CSF, macrophage colony stimulating factor; MMP, matrix metalloproteinase; NO, nitric oxide; PDGF, platelet‐derived growth factor; TGF‐β, transforming growth factor β; TNF‐α, tumor necrosis factor α. Cynthia S. Gordon © 2014 MedAnimations.com.
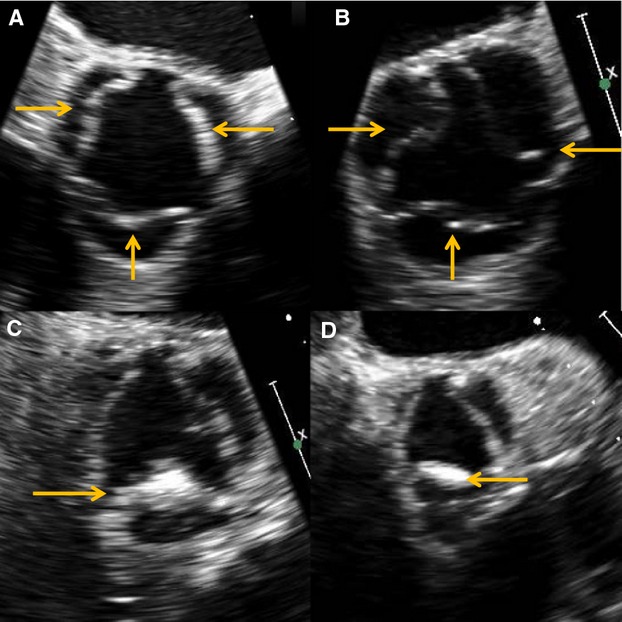
Patterns of aortic sclerosis seen on echocardiography. Diffuse (A) and mixed (B) types are associated with higher rates of coronary artery disease than are localized nodular (C) and localized nonnodular (D) forms. Arrows indicate areas of valvular sclerosis.
Similar articles
-
Thoracic aortic arteriosclerosis in patients with degenerative aortic stenosis with and without coexisting coronary artery disease.Ann Thorac Surg. 2008 Jan;85(1):113-9. doi: 10.1016/j.athoracsur.2007.08.025. Ann Thorac Surg. 2008. PMID: 18154793
-
Aortic root, not valve, calcification correlates with coronary artery calcification in patients with severe aortic stenosis: A two-center study.Atherosclerosis. 2015 Dec;243(2):631-7. doi: 10.1016/j.atherosclerosis.2015.10.014. Epub 2015 Oct 22. Atherosclerosis. 2015. PMID: 26551591
-
Additional value of associating aortic valve calcification to coronary calcium as a gatekeeper for coronary tomography angiography.BMC Cardiovasc Disord. 2015 Jul 1;15:61. doi: 10.1186/s12872-015-0058-5. BMC Cardiovasc Disord. 2015. PMID: 26130116 Free PMC article.
-
Pathophysiological coronary and microcirculatory flow alterations in aortic stenosis.Nat Rev Cardiol. 2018 Jul;15(7):420-431. doi: 10.1038/s41569-018-0011-2. Nat Rev Cardiol. 2018. PMID: 29713011 Review.
-
Cardiovascular morbidity and mortality in patients with aortic valve calcification: A systematic review and meta-analysis.J Cardiovasc Comput Tomogr. 2019 Jul-Aug;13(4):190-195. doi: 10.1016/j.jcct.2019.06.006. Epub 2019 Jun 11. J Cardiovasc Comput Tomogr. 2019. PMID: 31239172
Cited by
-
Risk of Myocardial Infarction in Patients With Aortic Stenosis: Insights From the VALVENOR Registry.JACC Adv. 2025 May;4(5):101707. doi: 10.1016/j.jacadv.2025.101707. Epub 2025 Apr 25. JACC Adv. 2025. PMID: 40286367 Free PMC article.
-
The Role of Trace Elements in Cardiovascular Diseases.Toxics. 2023 Nov 23;11(12):956. doi: 10.3390/toxics11120956. Toxics. 2023. PMID: 38133357 Free PMC article. Review.
-
Reducing Long-Term Mortality Post Transcatheter Aortic Valve Replacement Requires Systemic Differentiation of Patient-Specific Coronary Hemodynamics.J Am Heart Assoc. 2023 Jun 6;12(11):e029310. doi: 10.1161/JAHA.123.029310. Epub 2023 May 26. J Am Heart Assoc. 2023. PMID: 37232234 Free PMC article.
-
Trace elements in patients with aortic valve sclerosis.Ther Adv Cardiovasc Dis. 2021 Jan-Dec;15:1753944720985985. doi: 10.1177/1753944720985985. Ther Adv Cardiovasc Dis. 2021. PMID: 33627011 Free PMC article.
-
Impact of Oxidative Stress and Protein S-Glutathionylation in Aortic Valve Sclerosis Patients with Overt Atherosclerosis.J Clin Med. 2019 Apr 24;8(4):552. doi: 10.3390/jcm8040552. J Clin Med. 2019. PMID: 31022838 Free PMC article.
References
-
- Stewart BF, Siscovick D, Lind BK, Gardin JM, Gottdiener JS, Smith VE, Kitzman DW, Otto CM. Clinical factors associated with calcific aortic valve disease. Cardiovascular Health Study. J Am Coll Cardiol. 1997; 29:630-634. - PubMed
-
- Freeman RV, Otto CM. Spectrum of calcific aortic valve disease: pathogenesis, disease progression, and treatment strategies. Circulation. 2005; 111:3316-3326. - PubMed
-
- Losi MA, Brevetti G, Schiano V, Barbati G, Parisi V, Contaldi C, Chiacchio E, Cavallaro M, Carpinella G, Fundaliotis A, Betocchi S, Brevetti L, Chiariello M. Aortic valve sclerosis in patients with peripheral and/or coronary arterial disease. Echocardiography. 2010; 27:608-612. - PubMed
-
- Chandra HR, Goldstein JA, Choudhary N, O'Neill CS, George PB, Gangasani SR, Cronin L, Marcovitz PA, Hauser AM, O'Neill WW. Adverse outcome in aortic sclerosis is associated with coronary artery disease and inflammation. J Am Coll Cardiol. 2004; 43:169-175. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
