

Treosulfan-based conditioning and hematopoietic cell transplantation for nonmalignant diseases: a prospective multicenter trial
- PMID: 25196857
- PMCID: PMC4324724
- DOI: 10.1016/j.bbmt.2014.08.020
Treosulfan-based conditioning and hematopoietic cell transplantation for nonmalignant diseases: a prospective multicenter trial
Abstract
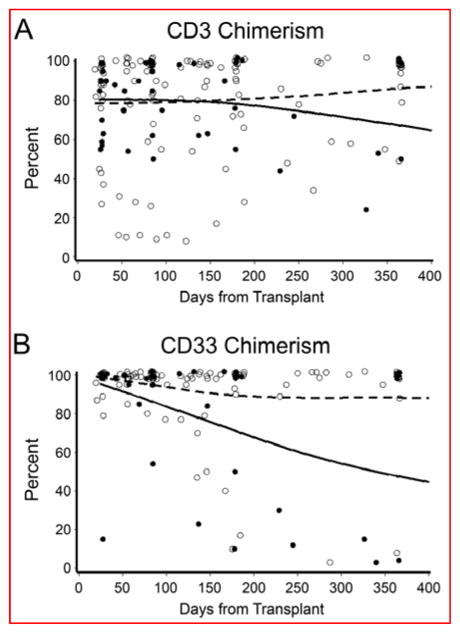
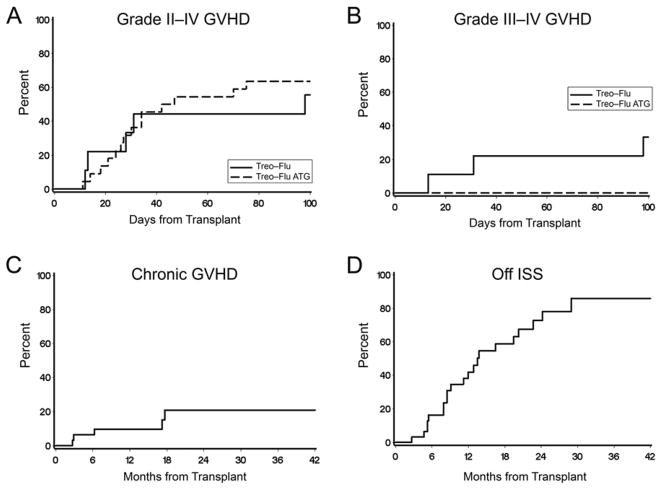
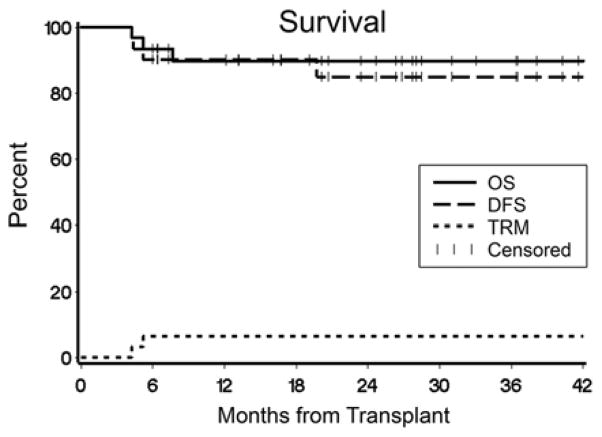
Hematopoietic cell transplantation is an effective treatment for patients with nonmalignant diseases and for many is the only known cure. Conventional myeloablative regimens have been associated with unacceptably high early transplant-related mortality (TRM), particularly in patients with comorbid conditions. This prospective multicenter trial was designed to determine the safety and engraftment efficacy of treosulfan-based conditioning in patients with nonmalignant diseases. Thirty-one patients received HLA-matched related (n = 4) or unrelated (n = 27) grafts after conditioning with treosulfan (total dose, 42 g/m(2)), fludarabine (total dose, 150 mg/m(2)), ± thymoglobulin (6 mg/kg; n = 22). Graft-versus-host disease (GVHD) prophylaxis consisted of tacrolimus and methotrexate. All patients engrafted. Day-100 TRM was 0%. With a median follow-up of 2 years, the 2-year survival was 90%. Three patients died of GVHD, recurrent hemophagocytic lymphohistiocytosis, and a surgical complication, respectively. The cumulative incidences of grades II to IV and III to IV acute GVHD at day 100 and chronic GVHD at 2 years were 62%, 10%, and 21%, respectively. Patients who received thymoglobulin had a significantly lower incidence of grades III to IV acute GVHD (0% versus 33%; P = .005). These results indicate that the combination of treosulfan, fludarabine, and thymoglobulin is effective at establishing donor engraftment with low toxicity and improved survival in patients with nonmalignant diseases and support the need for future disease-specific clinical trials.
Keywords: Allo-transplantation; Clinical results in inherited disorders; Conditioning regimen; Nonmalignant diseases; Reduced-intensity conditioning.
Copyright © 2014. Published by Elsevier Inc.
Conflict of interest statement
Figures
References
-
- Kahl C, Leisenring W, Deeg HJ, et al. Cyclophosphamide and antithymocyte globulin as a conditioning regimen for allogeneic marrow transplantation in patients with aplastic anaemia: a long-term follow-up. Br J Haematol. 2005;130:747–751. - PubMed
-
- Walters MC, Patience M, Leisenring W, et al. Bone marrow transplantation for sickle cell disease. N Engl J Med. 1996;335:369–376. - PubMed
-
- Kobayashi R, Ariga T, Nonoyama S, et al. Outcome in patients with Wiskott-Aldrich syndrome following stem cell transplantation: an analysis of 57 patients in Japan. Br J Haematol. 2006;135:362–366. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
