

Chest Radiographs for Pediatric TB Diagnosis: Interrater Agreement and Utility
- PMID: 25197271
- PMCID: PMC4150539
- DOI: 10.1155/2014/291841
Chest Radiographs for Pediatric TB Diagnosis: Interrater Agreement and Utility
Abstract
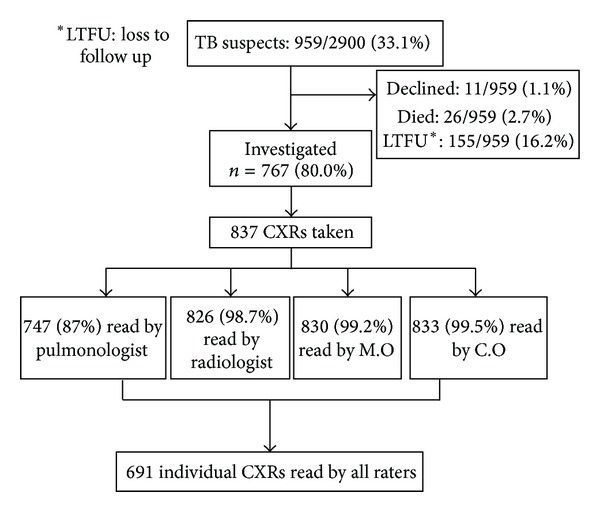
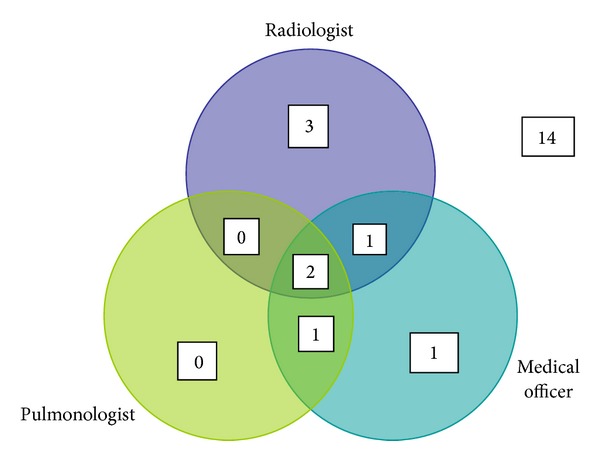
The chest radiograph (CXR) is considered a key diagnostic tool for pediatric tuberculosis (TB) in clinical management and endpoint determination in TB vaccine trials. We set out to compare interrater agreement for TB diagnosis in western Kenya. A pediatric pulmonologist and radiologist (experts), a medical officer (M.O), and four clinical officers (C.Os) with basic training in pediatric CXR reading blindly assessed CXRs of infants who were TB suspects in a cohort study. C.Os had access to clinical findings for patient management. Weighted kappa scores summarized interrater agreement on lymphadenopathy and abnormalities consistent with TB. Sensitivity and specificity of raters were determined using microbiologically confirmed TB as the gold standard (n = 8). A total of 691 radiographs were reviewed. Agreement on abnormalities consistent with TB was poor; k = 0.14 (95% CI: 0.10-0.18) and on lymphadenopathy moderate k = 0.26 (95% CI: 0.18-0.36). M.O [75% (95% CI: 34.9%-96.8%)] and C.Os [63% (95% CI: 24.5%-91.5%)] had high sensitivity for culture confirmed TB. TB vaccine trials utilizing expert agreement on CXR as a nonmicrobiologically confirmed endpoint will have reduced specificity and will underestimate vaccine efficacy. C.Os detected many of the bacteriologically confirmed cases; however, this must be interpreted cautiously as they were unblinded to clinical features.
Figures
References
-
- Schaaf HS, Beyers N, Gie RP, et al. Respiratory tuberculosis in childhood: the diagnostic value of clinical features and special investigations. Pediatric Infectious Disease Journal. 1995;14(3):189–194. - PubMed
-
- Jeena PM, Pillay P, Pillay T, Coovadia HM. Impact of HIV-1 co-infection on presentation and hospital-related mortality in children with culture proven pulmonary tuberculosis in Durban, South Africa. International Journal of Tuberculosis and Lung Disease. 2002;6(8):672–678. - PubMed
-
- Leung AN, Muller NL, Pineda PR, FitzGerald JM. Primary tuberculosis in childhood: radiographic manifestations. Radiology. 1992;182(1):87–91. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
