

Passive smoke exposure in chronic rhinosinusitis as assessed by hair nicotine
- PMID: 25197916
- PMCID: PMC4101130
- DOI: 10.2500/ajra.2014.28.4058
Passive smoke exposure in chronic rhinosinusitis as assessed by hair nicotine
Abstract
Background: Prevalence of passive smoke exposure is relatively unknown in chronic rhinosinusitis (CRS). Previous studies have attempted to establish this relationship using subjective, questionnaire-based methodologies to assess smoke exposure, thus introducing the potential for error bias. The purpose of this study was to accurately determine the prevalence of passive smoke exposure in CRS and control patients using hair nicotine levels as a quantitative measure of cigarette smoke exposure.
Methods: Hair samples were obtained at time of surgery from 569 patients: 404 undergoing surgery for CRS and 165 controls undergoing surgery for repair of cerebrospinal fluid leak, removal of pituitary tumors, or adenoidectomy from 2007 to 2013. Patient charts were reviewed for reported smoking status. Hair nicotine was quantified using reversed-phase high-performance liquid chromatography. Nonsmoking patients were classified as passive smoke exposed or smoke naïve according to the hair nicotine results. Statistical analysis was performed to test for differences in demographic information and smoke exposure prevalence between CRS, CRS subtypes, and controls.
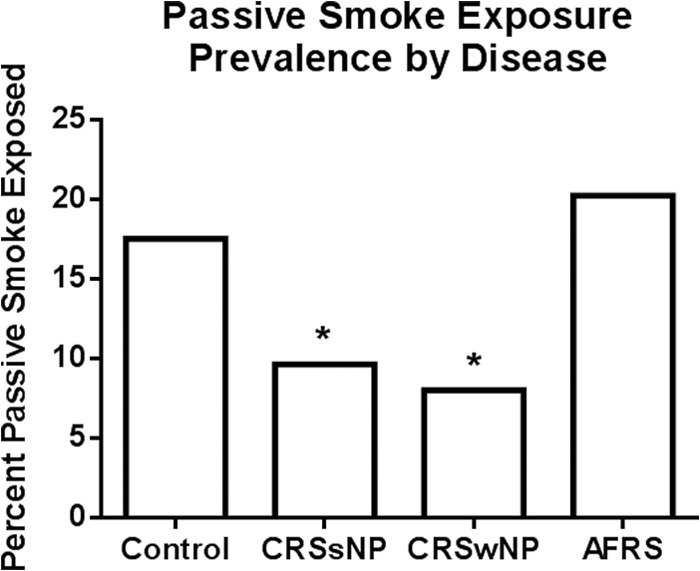
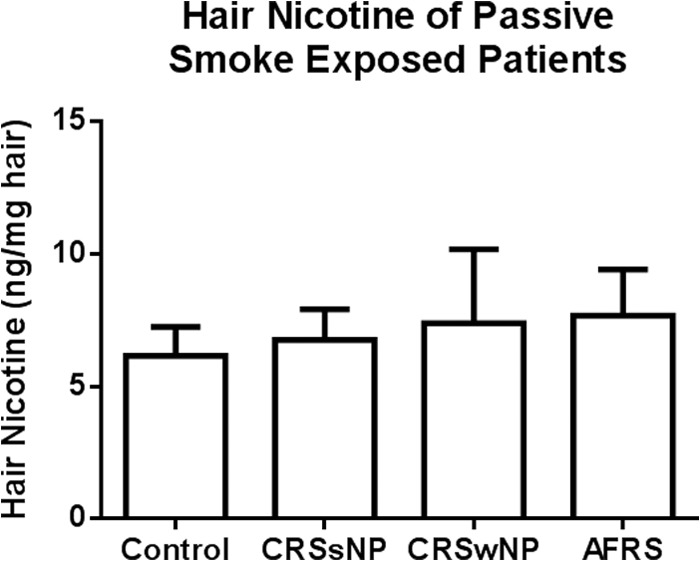
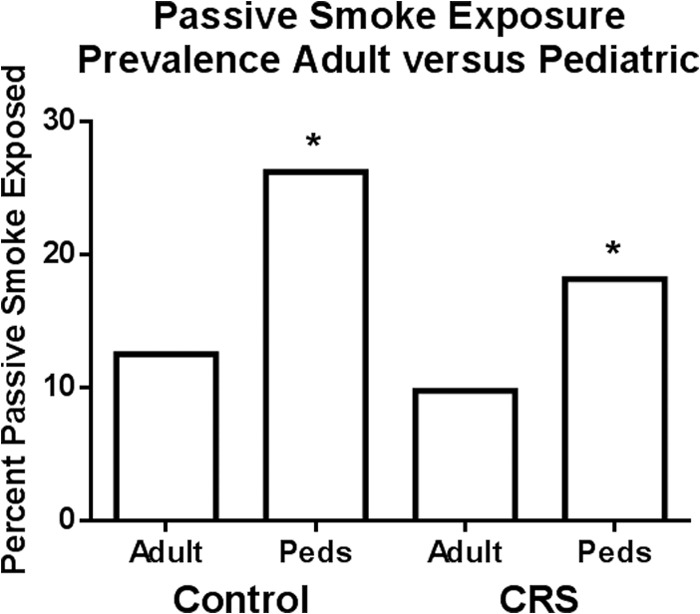
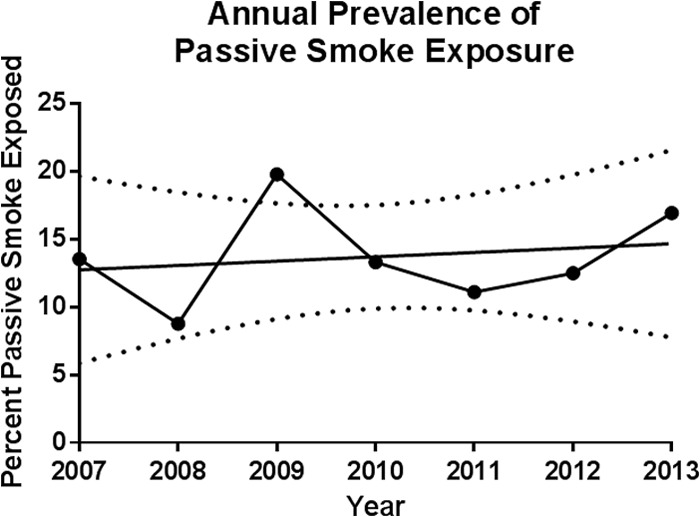
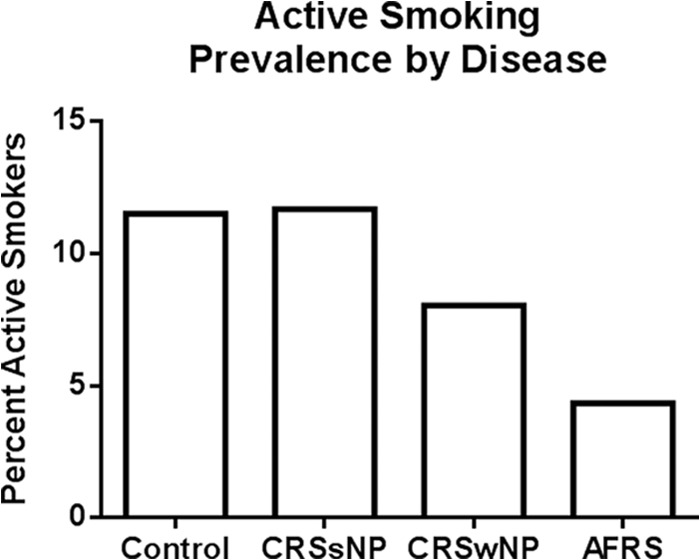
Results: The prevalence of passive smoke exposure in CRS as documented by hair nicotine was lower than previously reported subjective estimates. Passive smoke exposure rates were equivalent between those with CRS versus controls and significantly higher in children. Severity of passive smoke exposure was also equivalent between CRS subsets and controls. Annual passive smoke exposure prevalence did not change over time.
Conclusion: There is no clear evidence of avoidance of passive smoke exposure in the CRS population compared with controls. Passive smoke exposure also remained stable over time despite recent regional implementation of smoking bans. Given the constancy of exposure, it is critical that the impact of passive smoke on CRS exacerbation, outcomes, and pathophysiology be evaluated in large-scale clinical studies.
Conflict of interest statement
The authors have no conflicts of interest to declare pertaining to this article
Figures
References
-
- Gliklich RE, Metson R. The health impact of chronic sinusitis in patients seeking otolaryngologic care. Otolaryngol Head Neck Surg 113:104–109, 1995. - PubMed
-
- Chen Y, Dales R, Lin M. The epidemiology of chronic rhinosinusitis in Canadians. Laryngoscope 113:1199–1205, 2003. - PubMed
-
- Hastan D, Fokkens WJ, Bachert C, et al. Chronic rhinosinusitis in Europe—An underestimated disease. A GA2LEN study. Allergy 66:1216–1223, 2011. - PubMed
-
- Fokkens WJ, Lund VJ, Mullol J, et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology 50:1–12, 2012. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
