

Rethinking composite end points in clinical trials: insights from patients and trialists
- PMID: 25200210
- PMCID: PMC4275445
- DOI: 10.1161/CIRCULATIONAHA.113.006588
Rethinking composite end points in clinical trials: insights from patients and trialists
Abstract
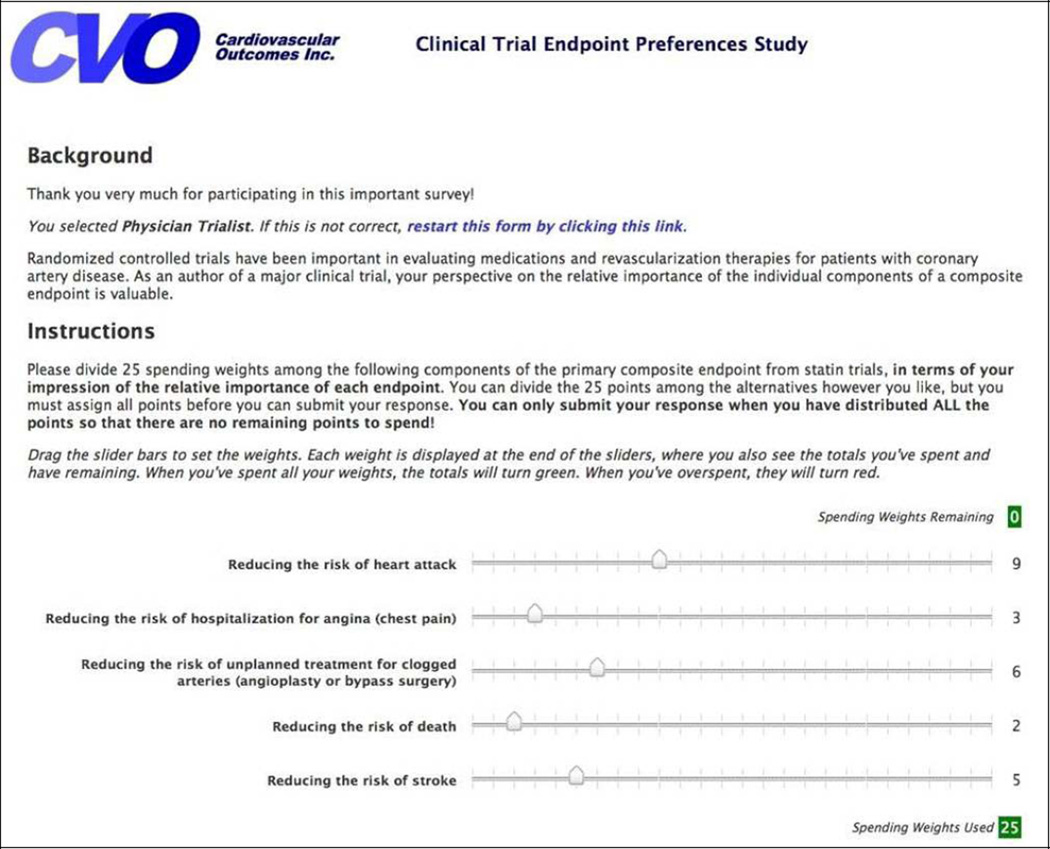
Background: Many clinical trials use composite end points to reduce sample size, but the relative importance of each individual end point within the composite may differ between patients and researchers.
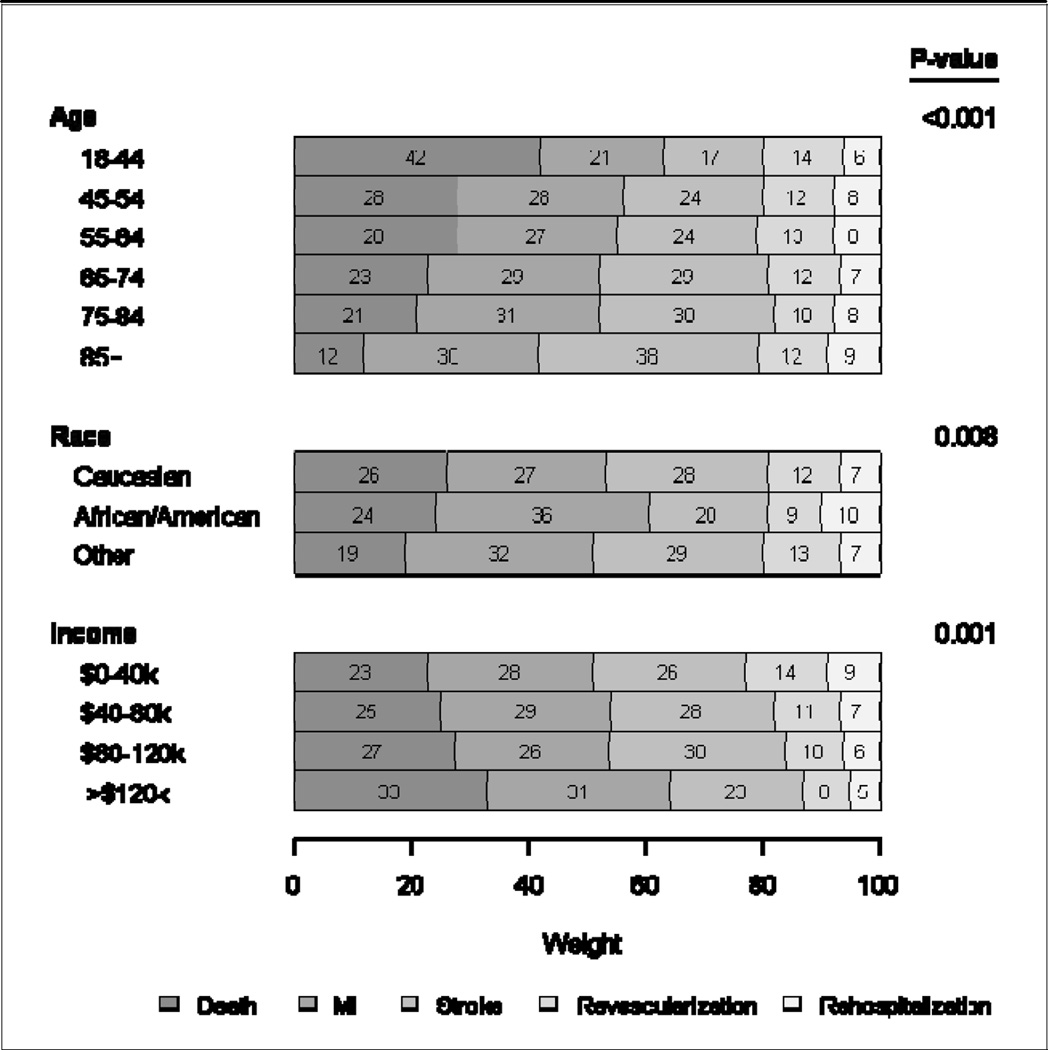
Methods and results: We asked 785 cardiovascular patients and 164 clinical trial authors to assign 25 "spending weights" across 5 common adverse events comprising composite end points in cardiovascular trials: death, myocardial infarction, stroke, coronary revascularization, and hospitalization for angina. We then calculated end point ratios for each participant's ratings of each nonfatal end point relative to death. Whereas patients assigned an average weight of 5 to death, equal or greater weight was assigned to myocardial infarction (mean ratio, 1.12) and stroke (ratio, 1.08). In contrast, clinical trialists were much more concerned about death (average weight, 8) than myocardial infarction (ratio, 0.63) or stroke (ratio, 0.53). Both patients and trialists considered revascularization (ratio, 0.48 and 0.20, respectively) and hospitalization (ratio, 0.28 and 0.13, respectively) as substantially less severe than death. Differences between patient and trialist end point weights persisted after adjustment for demographic and clinical characteristics (P<0.001 for all comparisons).
Conclusions: Patients and clinical trialists did not weigh individual components of a composite end point equally. Whereas trialists are most concerned about avoiding death, patients place equal or greater importance on reducing myocardial infarction or stroke. Both groups considered revascularization and hospitalization as substantially less severe. These findings suggest that equal weights in a composite clinical end point do not accurately reflect the preferences of either patients or trialists.
Keywords: cardiovascular diseases; clinical trial; end point determination; patient preference; patient-centered care; statistics.
© 2014 American Heart Association, Inc.
Figures
Comment in
-
Patient-centered outcomes composites: a glimpse of the future.Circulation. 2014 Oct 7;130(15):1223-4. doi: 10.1161/CIRCULATIONAHA.114.013135. Epub 2014 Sep 8. Circulation. 2014. PMID: 25200211 No abstract available.
References
-
- Freemantle N, Calvert M, Wood J, Eastaugh J, Griffin C. Composite outcomes in randomized trials: Greater precision but with greater uncertainty? JAMA. 2003;289:2554–2559. - PubMed
-
- Cannon CP, Sharis PJ, Schweiger MJ, McCabe CH, Diver DJ, Shah PK, Sequeira RF, Greene RM, Perritt RL, Poole WK, Braunwald E. Prospective validation of a composite end point in thrombolytic trials of acute myocardial infarction (timi 4 and 5). Thrombosis in myocardial infarction. Am J Cardiol. 1997;80:696–699. - PubMed
-
- Califf RM, Harrelson-Woodlief L, Topol EJ. Left ventricular ejection fraction may not be useful as an end point of thrombolytic therapy comparative trials. Circulation. 1990;82:1847–1853. - PubMed
-
- Kaul S, Diamond GA. Trial and error. How to avoid commonly encountered limitations of published clinical trials. J Am Coll Cardiol. 2010;55:415–427. - PubMed
-
- Kip KE, Hollabaugh K, Marroquin OC, Williams DO. The problem with composite end points in cardiovascular studies: The story of major adverse cardiac events and percutaneous coronary intervention. J Am Coll Cardiol. 2008;51:701–707. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
