

Individuals with transtibial limb loss use interlimb force asymmetries to maintain multi-directional reactive balance control
- PMID: 25200883
- PMCID: PMC4337775
- DOI: 10.1016/j.clinbiomech.2014.08.007
Individuals with transtibial limb loss use interlimb force asymmetries to maintain multi-directional reactive balance control
Abstract
Background: Deficits in balance control are one of the most common and serious mobility challenges facing individuals with lower limb loss. Yet, dynamic postural balance control among individuals with lower limb loss remains poorly understood. Here we examined the kinematics and kinetics of dynamic balance in individuals with unilateral transtibial limb loss.
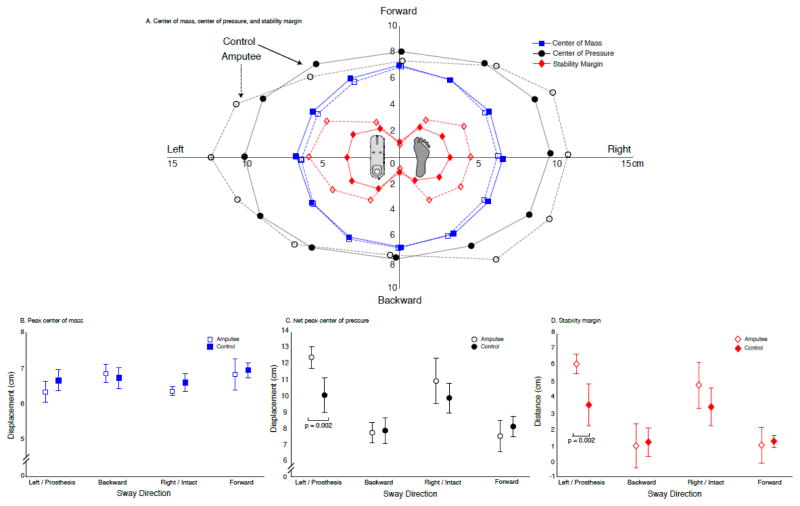
Methods: Five individuals with unilateral transtibial limb loss, and five age- and gender-matched controls completed a series of randomly applied multi-directional support surface translations. Whole-body metrics, e.g. peak center-of-mass displacement and net center-of-pressure displacement were compared across cohorts. Stability margin was computed as the difference between peak center-of-pressure and center-of-mass displacement. Additionally, center-of-pressure and ground reaction force magnitude and direction were compared between the prosthetic, intact, and control legs.
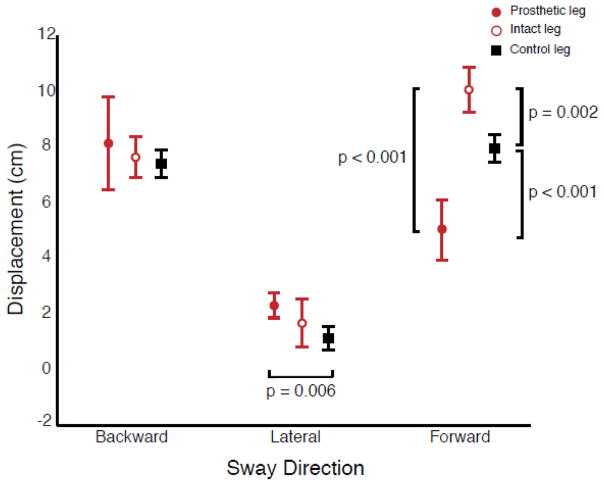
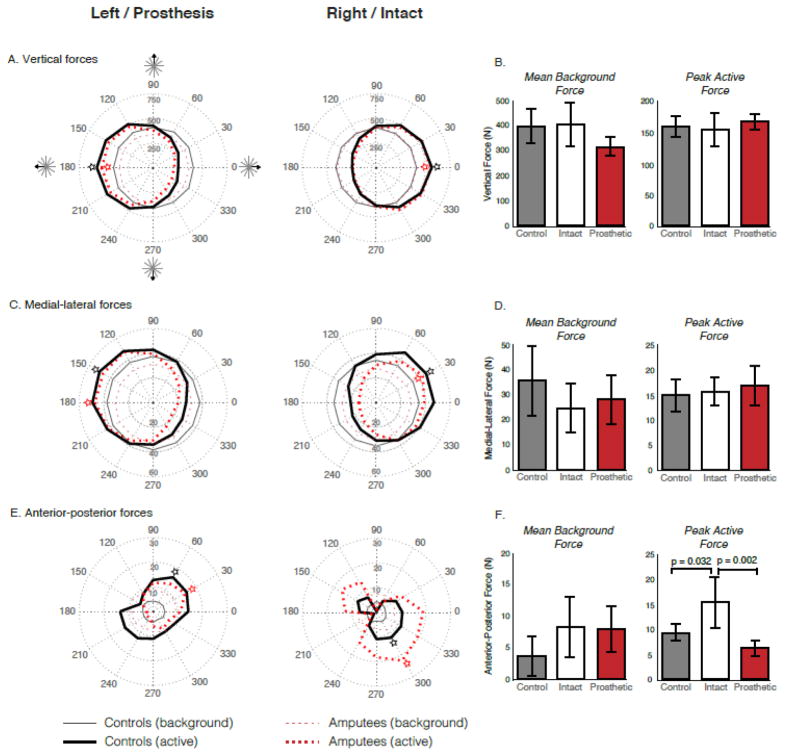
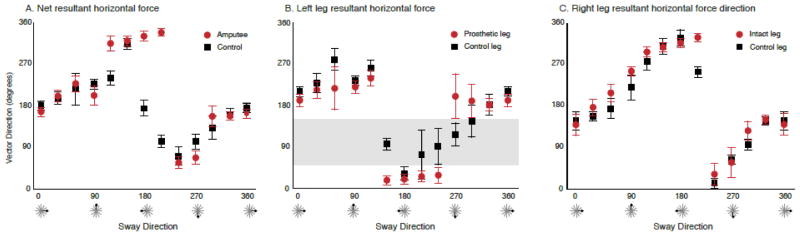
Findings: Peak center-of-mass displacement and stability margin did not differ between individuals with transtibial limb loss and controls for all perturbation directions except those loading only the prosthetic leg; in such cases the stability margin was actually larger than controls. Despite similar center-of-mass displacement, greater center-of-pressure displacement was observed in the intact leg during anterior-posterior perturbations, and under the prosthetic leg in medial-lateral perturbations. Further, in the prosthetic leg, ground reaction forces were smaller and spanned fewer directions.
Interpretation: Deficits in balance control among individuals with transtibial limb loss may be due to their inability to use their prosthetic leg to generate forces that are equal in magnitude and direction to those of unimpaired adults. Targeting this force-generating deficit through technological or rehabilitation innovations may improve balance control.
Keywords: Amputee; Artificial limb; Feedback; Ground reaction force; Posture; Stability.
Copyright © 2014 Elsevier Ltd. All rights reserved.
Figures

References
-
- Jayakaran P, Johnson GM, Sullivan SJ, Nitz JC. Instrumented measurement of balance and postural control in individuals with lower limb amputation. Int J of Rehabil Res. 2012;35:187–196. - PubMed
-
- Miller WC, Speechley M, Deathe B. The prevalence and risk factors of falling and fear of falling among lower extremity amputees. Arch Phys Med Rehab. 2001;82:1031–1037. - PubMed
-
- Ülger Ö, Topuz S, Bayramlar K. Risk factors, frequency, and causes of falling in geriatric persons who has had a limb removed by amputation. Top Geriatr Rehabil. 2010;26:156–163.
-
- van Velzen JM, van Bennekom CA, Polomski W, Slootman JR, van der Woude LH, Houdijk H. Physical capacity and walking ability after lower limb amputation: a systematic review. Clin Rehabil. 2006;20:999–1016. - PubMed
-
- McWhinnie DL, Gordon AC, Collin J. Rehabilitation outcome 5 years after 100 lower-limb amputations. Br J Surg. 1994;81:1596–1599. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
