

Tissue-engineering-based strategies for regenerative endodontics
- PMID: 25201917
- PMCID: PMC4237634
- DOI: 10.1177/0022034514549809
Tissue-engineering-based strategies for regenerative endodontics
Abstract
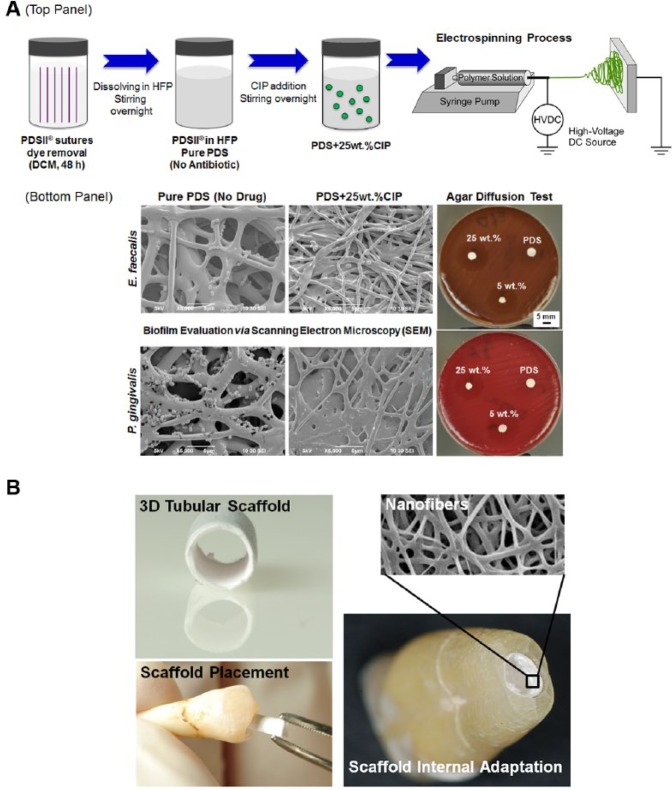
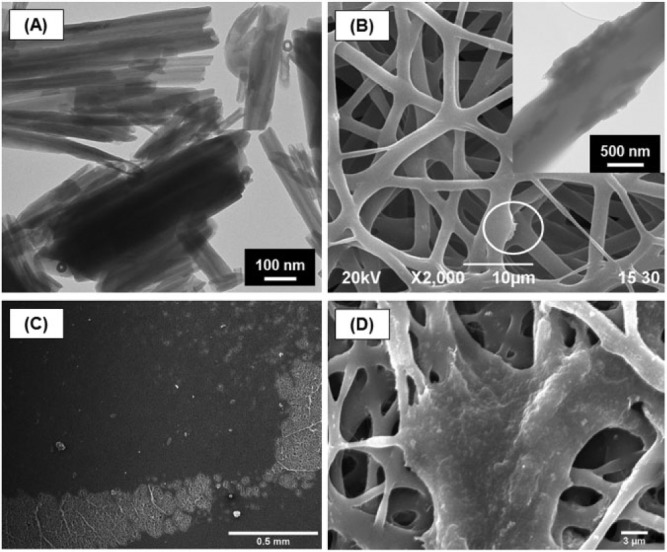
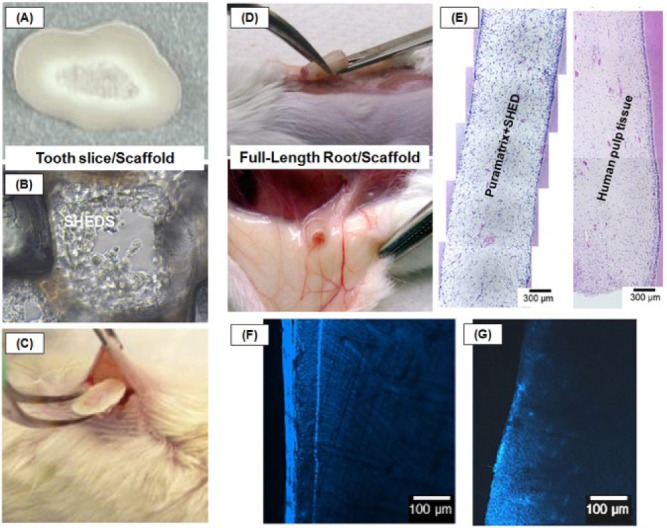
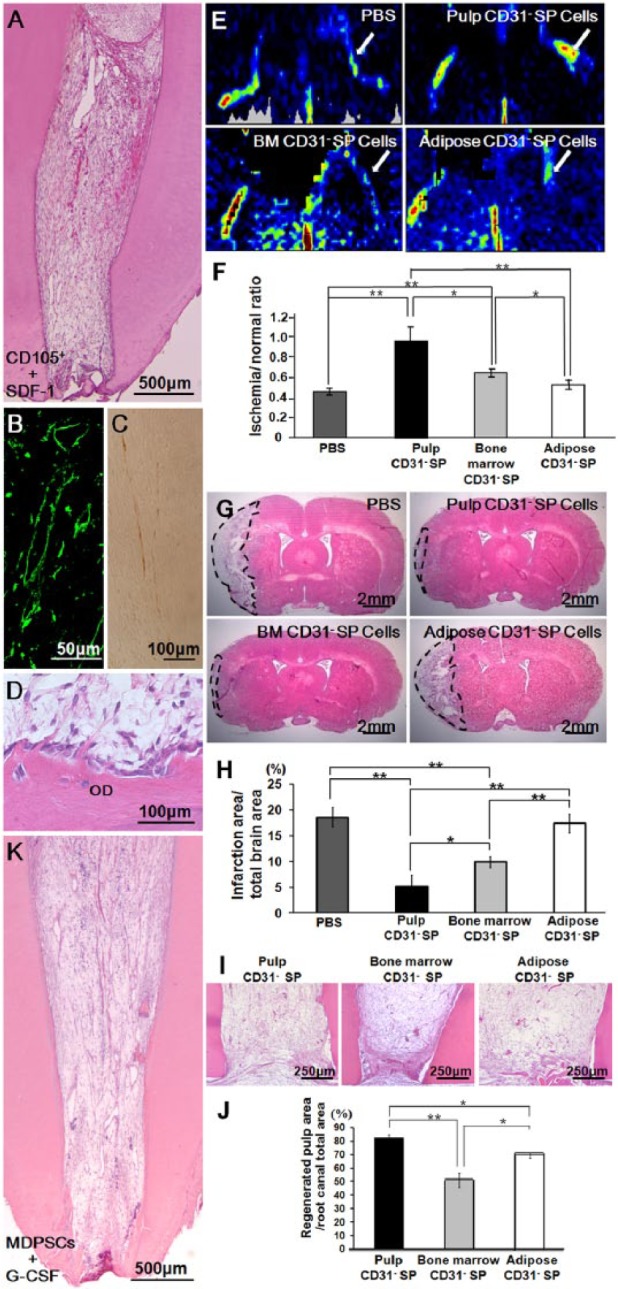
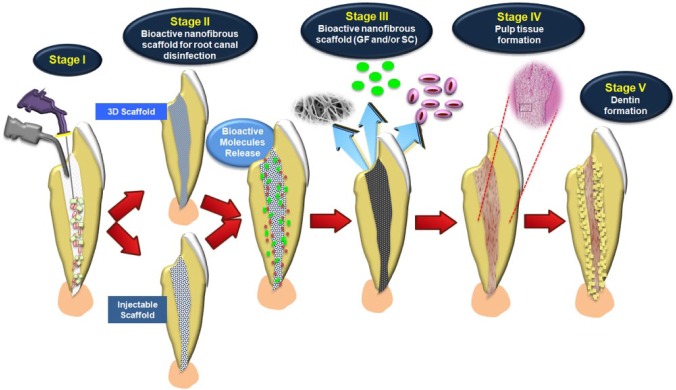
Stemming from in vitro and in vivo pre-clinical and human models, tissue-engineering-based strategies continue to demonstrate great potential for the regeneration of the pulp-dentin complex, particularly in necrotic, immature permanent teeth. Nanofibrous scaffolds, which closely resemble the native extracellular matrix, have been successfully synthesized by various techniques, including but not limited to electrospinning. A common goal in scaffold synthesis has been the notion of promoting cell guidance through the careful design and use of a collection of biochemical and physical cues capable of governing and stimulating specific events at the cellular and tissue levels. The latest advances in processing technologies allow for the fabrication of scaffolds where selected bioactive molecules can be delivered locally, thus increasing the possibilities for clinical success. Though electrospun scaffolds have not yet been tested in vivo in either human or animal pulpless models in immature permanent teeth, recent studies have highlighted their regenerative potential both from an in vitro and in vivo (i.e., subcutaneous model) standpoint. Possible applications for these bioactive scaffolds continue to evolve, with significant prospects related to the regeneration of both dentin and pulp tissue and, more recently, to root canal disinfection. Nonetheless, no single implantable scaffold can consistently guide the coordinated growth and development of the multiple tissue types involved in the functional regeneration of the pulp-dentin complex. The purpose of this review is to provide a comprehensive perspective on the latest discoveries related to the use of scaffolds and/or stem cells in regenerative endodontics. The authors focused this review on bioactive nanofibrous scaffolds, injectable scaffolds and stem cells, and pre-clinical findings using stem-cell-based strategies. These topics are discussed in detail in an attempt to provide future direction and to shed light on their potential translation to clinical settings.
Keywords: dental pulp; dentin; nanofibers; regeneration; stem cells; tissue scaffolds.
© International & American Associations for Dental Research.
Conflict of interest statement
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.
Figures
References
-
- Akkouch A, Zhang Z, Rouabhia M. (2013). Engineering bone tissue using human dental pulp stem cells and an osteogenic collagen-hydroxyapatite-poly (L-lactide-co-ϵ-caprolactone) scaffold. J Biomater Appl 28:922-936. - PubMed
-
- Banchs F, Trope M. (2004). Revascularization of immature permanent teeth with apical periodontitis: new treatment protocol? J Endod 30:196-200. - PubMed
-
- Baylan N, Bhat S, Ditto M, Lawrence JG, Lecka-Czernik B, Yildirim-Ayan E. (2013). Polycaprolactone nanofiber interspersed collagen type-I scaffold for bone regeneration: a unique injectable osteogenic scaffold. Biomed Mater 8:045011. - PubMed
-
- Becerra P, Ricucci D, Loghin S, Gibbs JL, Lin LM. (2014). Histologic study of a human immature permanent premolar with chronic apical abscess after revascularization/revitalization. J Endod 40:133-139. - PubMed
-
- Bose R, Nummikoski P, Hargreaves K. (2009). A retrospective evaluation of radiographic outcomes in immature teeth with necrotic root canal systems treated with regenerative endodontic procedures. J Endod 35:1343-1349. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
