

Extent of surgery for papillary thyroid cancer is not associated with survival: an analysis of 61,775 patients
- PMID: 25203876
- PMCID: PMC4532384
- DOI: 10.1097/SLA.0000000000000925
Extent of surgery for papillary thyroid cancer is not associated with survival: an analysis of 61,775 patients
Abstract
Objective: To examine the association between the extent of surgery and overall survival in a large contemporary cohort of patients with papillary thyroid cancer (PTC).
Background: Guidelines recommend total thyroidectomy for PTC tumors >1 cm, based on older data demonstrating an overall survival advantage for total thyroidectomy over lobectomy.
Methods: Adult patients with PTC tumors 1.0-4.0 cm undergoing thyroidectomy in the National Cancer Database, 1998-2006, were included. Cox proportional hazards models were applied to measure the association between the extent of surgery and overall survival while adjusting for patient demographic and clinical factors, including comorbidities, extrathyroidal extension, multifocality, nodal and distant metastases, and radioactive iodine treatment.
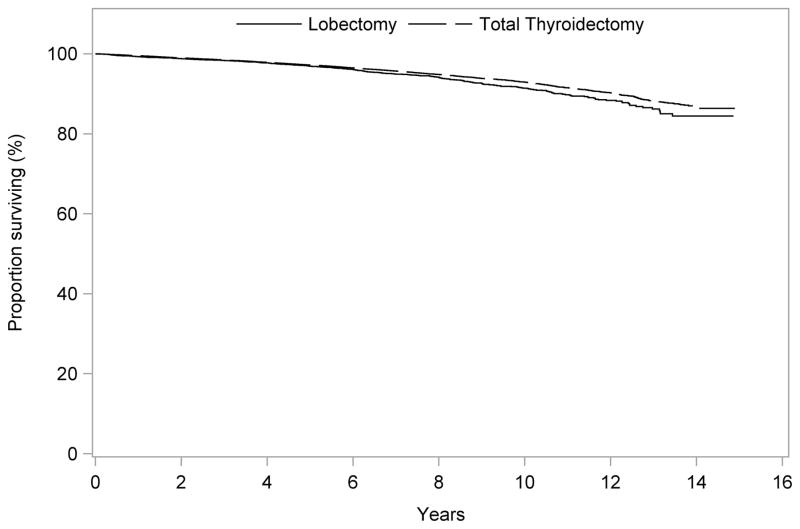
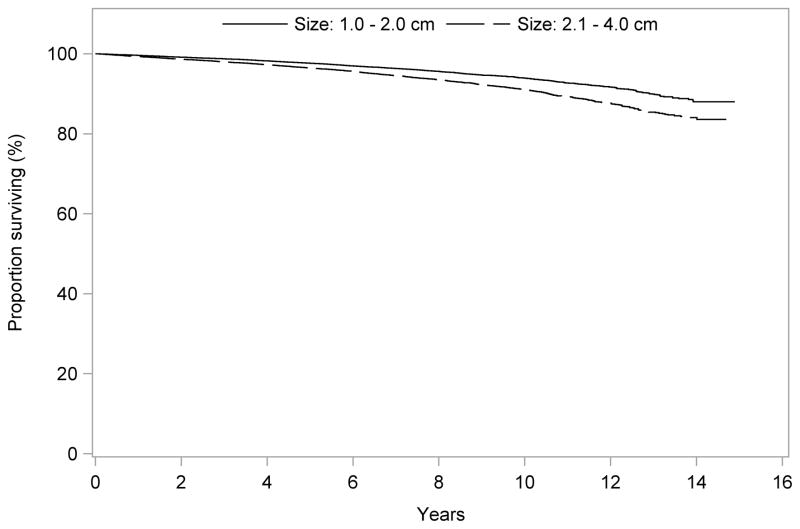
Results: Among 61,775 PTC patients, 54,926 underwent total thyroidectomy and 6849 lobectomy. Compared with lobectomy, patients undergoing total thyroidectomy had more nodal (7% vs 27%), extrathyroidal (5% vs 16%), and multifocal disease (29% vs 44%) (all Ps < 0.001). Median follow-up was 82 months (range, 60-179 months). After multivariable adjustment, overall survival was similar in patients undergoing total thyroidectomy versus lobectomy for tumors 1.0-4.0 cm [hazard ratio (HR) = 0.96; 95% confidence interval (CI), 0.84-1.09); P = 0.54] and when stratified by tumor size: 1.0-2.0 cm [HR = 1.05; 95% CI, 0.88-1.26; P = 0.61] and 2.1-4.0 cm [HR = 0.89; 95% CI, 0.73-1.07; P = 0.21]. Older age, male sex, black race, lower income, tumor size, and presence of nodal or distant metastases were independently associated with compromised survival (P < 0.0001).
Conclusions: Current guidelines suggest total thyroidectomy for PTC tumors >1 cm. However, we did not observe a survival advantage associated with total thyroidectomy compared with lobectomy. These findings call into question whether tumor size should be an absolute indication for total thyroidectomy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- American Cancer Society. [Accessed March 01, 2014];Cancer Facts & Figures. 2013 Available at: http://www.cancer.org/acs/groups/content/@epidemiologysurveilance/docume....
-
- Siegel R, DeSantis C, Virgo K, et al. Cancer treatment and survivorship statistics, 2012. CA Cancer J Clin. 2012;62:220–241. - PubMed
-
- Davies L, Welch HG. Thyroid cancer survival in the United States: observational data from 1973 to 2005. Arch Otolaryngol Head Neck Surg. 2010;136:440–444. - PubMed
-
- Cooper DS, Doherty GM, Haugen BR, et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid. 2009;19:1167–1214. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
