

Mortality in patients with HIV-1 infection starting antiretroviral therapy in South Africa, Europe, or North America: a collaborative analysis of prospective studies
- PMID: 25203931
- PMCID: PMC4159124
- DOI: 10.1371/journal.pmed.1001718
Mortality in patients with HIV-1 infection starting antiretroviral therapy in South Africa, Europe, or North America: a collaborative analysis of prospective studies
Abstract
Background: High early mortality in patients with HIV-1 starting antiretroviral therapy (ART) in sub-Saharan Africa, compared to Europe and North America, is well documented. Longer-term comparisons between settings have been limited by poor ascertainment of mortality in high burden African settings. This study aimed to compare mortality up to four years on ART between South Africa, Europe, and North America.
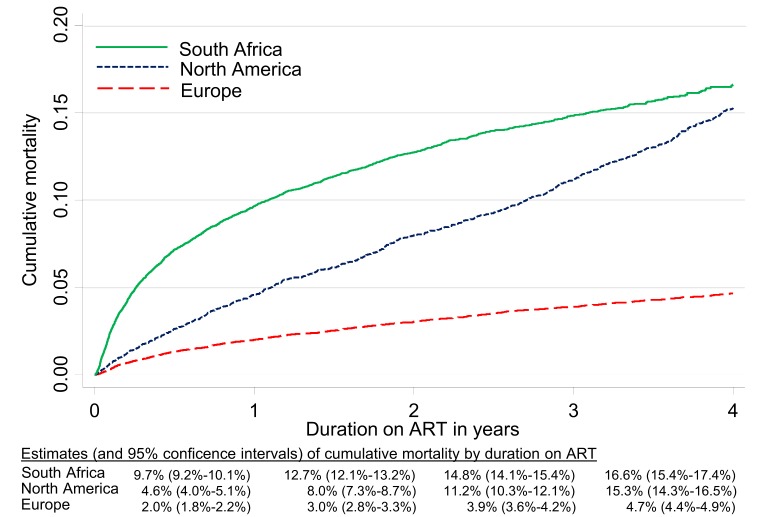
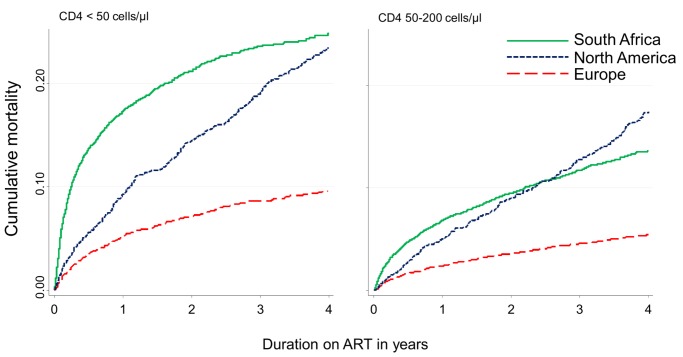
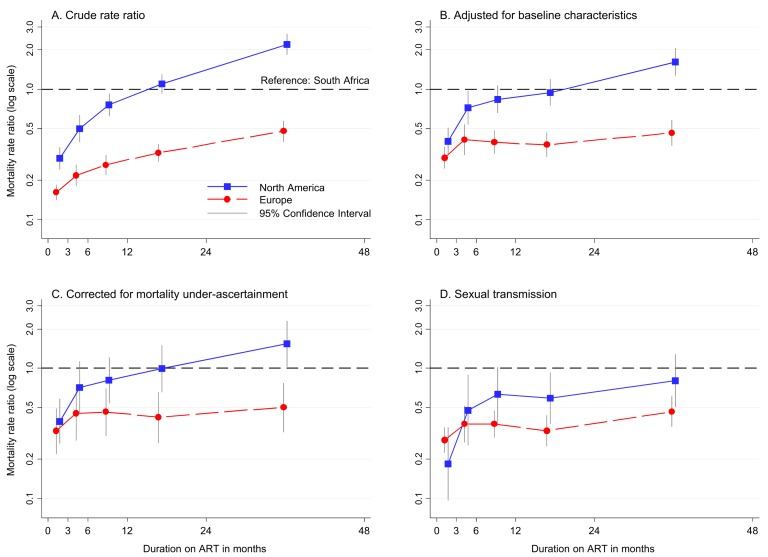
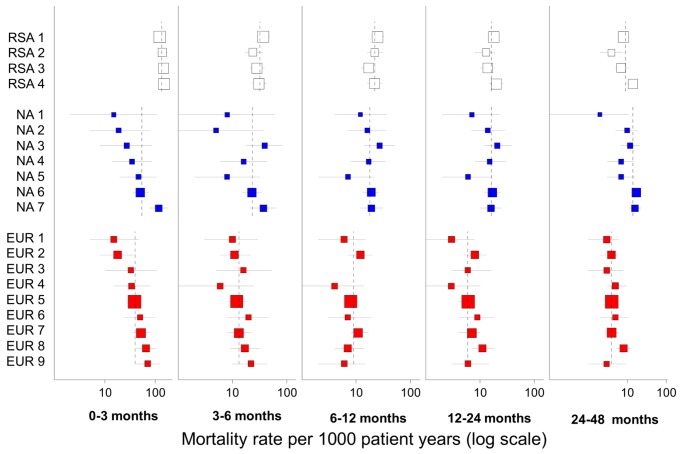
Methods and findings: Data from four South African cohorts in which patients lost to follow-up (LTF) could be linked to the national population register to determine vital status were combined with data from Europe and North America. Cumulative mortality, crude and adjusted (for characteristics at ART initiation) mortality rate ratios (relative to South Africa), and predicted mortality rates were described by region at 0-3, 3-6, 6-12, 12-24, and 24-48 months on ART for the period 2001-2010. Of the adults included (30,467 [South Africa], 29,727 [Europe], and 7,160 [North America]), 20,306 (67%), 9,961 (34%), and 824 (12%) were women. Patients began treatment with markedly more advanced disease in South Africa (median CD4 count 102, 213, and 172 cells/µl in South Africa, Europe, and North America, respectively). High early mortality after starting ART in South Africa occurred mainly in patients starting ART with CD4 count <50 cells/µl. Cumulative mortality at 4 years was 16.6%, 4.7%, and 15.3% in South Africa, Europe, and North America, respectively. Mortality was initially much lower in Europe and North America than South Africa, but the differences were reduced or reversed (North America) at longer durations on ART (adjusted rate ratios 0.46, 95% CI 0.37-0.58, and 1.62, 95% CI 1.27-2.05 between 24 and 48 months on ART comparing Europe and North America to South Africa). While bias due to under-ascertainment of mortality was minimised through death registry linkage, residual bias could still be present due to differing approaches to and frequency of linkage.
Conclusions: After accounting for under-ascertainment of mortality, with increasing duration on ART, the mortality rate on HIV treatment in South Africa declines to levels comparable to or below those described in participating North American cohorts, while substantially narrowing the differential with the European cohorts. Please see later in the article for the Editors' Summary.
Conflict of interest statement
MSS is the local principal investigator on studies sponsored by Abbvie, Gilead, BMS, Merck, BI, ViiV, and Jannsen, where funding goes directly to the institution but not to MSS. PR, through his institution, has received independent scientific grant support from Gilead Sciences, Janssen Pharmaceutica N.V., Merck&Co, Bristol-Myers Squibb, and ViiV Healthcare, and travel support through his institution from Gilead Sciences and Janssen Pharmaceutica N.V. In addition, PR has served on a scientific advisory board for Gilead Sciences and serves on a data safety monitoring committee for Janssen Pharmaceutica N.V., for which his institution has received remuneration. KE has received honoraria from Abbott for educational lectures. JS has received research grants from the UK Medical Research Council. JS has received payment from Gilead Sciences, Inc for educational presentations.
Figures
Comment in
-
Convergence of mortality rates among patients on antiretroviral therapy in South Africa and North America.PLoS Med. 2014 Sep 9;11(9):e1001719. doi: 10.1371/journal.pmed.1001719. eCollection 2014 Sep. PLoS Med. 2014. PMID: 25202913 Free PMC article.
References
-
- Bekker LG, Orrell C, Reader L, Matoti K, Cohen K, et al. (2003) Antiretroviral therapy in a community clinic–early lessons from a pilot project. S Afr Med J 93: 458–462. - PubMed
-
- Coetzee D, Hildebrand K, Boulle A, Maartens G, Louis F, et al. (2004) Outcomes after two years of providing antiretroviral treatment in Khayelitsha, South Africa. AIDS 18: 887–895. - PubMed
-
- Wester CW, Kim S, Bussmann H, Avalos A, Ndwapi N, et al. (2005) Initial response to highly active antiretroviral therapy in HIV-1C-infected adults in a public sector treatment program in Botswana. JAIDS 40: 336–343. - PubMed
-
- Stringer JS, Zulu I, Levy J, Stringer EM, Mwango A, et al. (2006) Rapid scale-up of antiretroviral therapy at primary care sites in Zambia: feasibility and early outcomes. JAMA 296: 782–793. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P30 AI027767/AI/NIAID NIH HHS/United States
- P30 AI054999/AI/NIAID NIH HHS/United States
- CAPMC/ CIHR/Canada
- U10-AA13566/AA/NIAAA NIH HHS/United States
- MR/J002380/1/MRC_/Medical Research Council/United Kingdom
- U01 AA020790/AA/NIAAA NIH HHS/United States
- P30 AI027757/AI/NIAID NIH HHS/United States
- P30-AI027767/AI/NIAID NIH HHS/United States
- G0700820/MRC_/Medical Research Council/United Kingdom
- 5U01AI069924-05/AI/NIAID NIH HHS/United States
- P30 AI54999/AI/NIAID NIH HHS/United States
- U10 AA013566/AA/NIAAA NIH HHS/United States
- U24-AA020794/AA/NIAAA NIH HHS/United States
- U01 AI069924/AI/NIAID NIH HHS/United States
- U24 AA020794/AA/NIAAA NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
