

Four phases of intravenous fluid therapy: a conceptual model
- PMID: 25204700
- PMCID: PMC6863743
- DOI: 10.1093/bja/aeu300
Four phases of intravenous fluid therapy: a conceptual model
Abstract
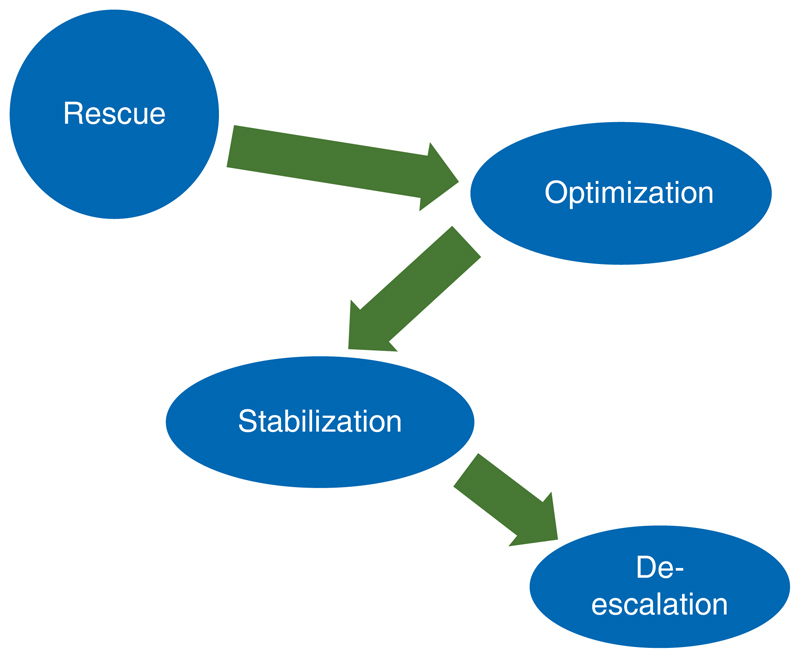
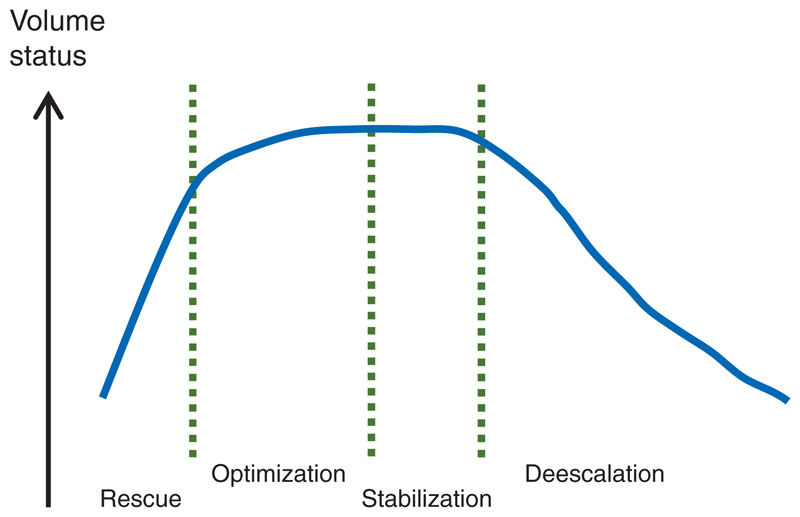
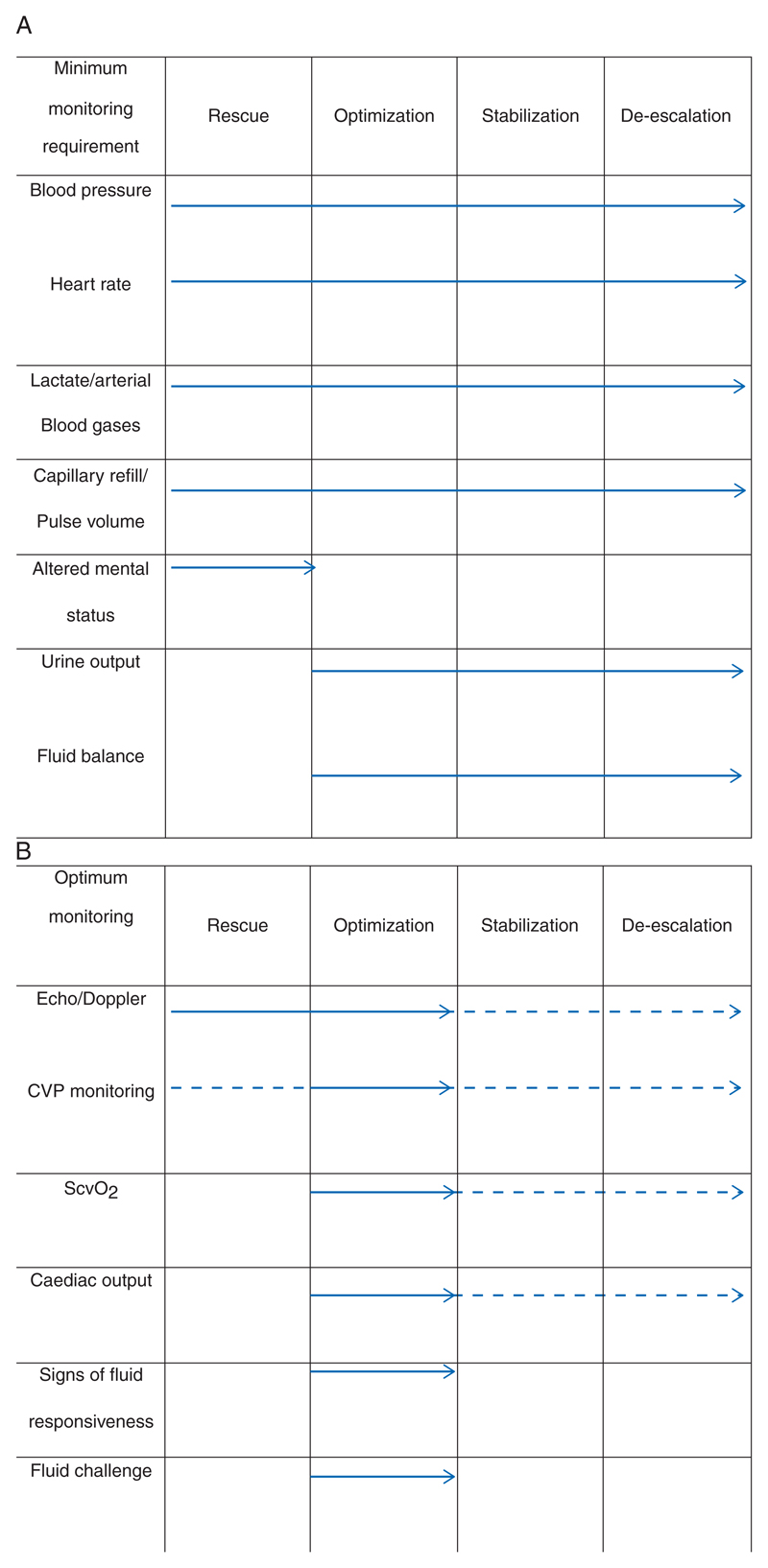
I.V. fluid therapy plays a fundamental role in the management of hospitalized patients. While the correct use of i.v. fluids can be lifesaving, recent literature demonstrates that fluid therapy is not without risks. Indeed, the use of certain types and volumes of fluid can increase the risk of harm, and even death, in some patient groups. Data from a recent audit show us that the inappropriate use of fluids may occur in up to 20% of patients receiving fluid therapy. The delegates of the 12th Acute Dialysis Quality Initiative (ADQI) Conference sought to obtain consensus on the use of i.v. fluids with the aim of producing guidance for their use. In this article, we review a recently proposed model for fluid therapy in severe sepsis and propose a framework by which it could be adopted for use in most situations where fluid management is required. Considering the dose-effect relationship and side-effects of fluids, fluid therapy should be regarded similar to other drug therapy with specific indications and tailored recommendations for the type and dose of fluid. By emphasizing the necessity to individualize fluid therapy, we hope to reduce the risk to our patients and improve their outcome.
Keywords: adults; critical care; fluid therapy; resuscitation.
© The Author 2014. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Conflict of interest statement
E.H. has received speakers fees from Astute Medical and Pfizer. C.S.B. received honoraria from Phoenix medical, Hospira, Orion, Covidien, and LiDCO, and functioned in the advisory board of Grifols. R.M. consulted for Baxter, Grifols, Abbvie, Gambro, Takeda, Astute, Astellas, GSK, CSL Behring, and Eli-Lilly. J.A.K. has received grant support from Baxter, and serves as a paid consultant for Baxter and Grifols. M.G.M. has received honoraria for speaking/consultation and/or travel expenses from Baxter, BBraun, Covidien, Fresenius-Kabi, Hospira, LidCo, and as a consultant to AQIX (start up company with a novel crystalloid solution-pre-clinical). He is a director of Medical Defence Technologies LLC (“Gastrostim” patented) and a coinventor of “QUENCH” IP being exploited by UCL Business. M.G.M.’s chair at UCL is endowed by Smiths Medical Ltd and this company provide charitable donations to the department on an annual basis. Deltex Medical also provide unrestricted grant funds to M.G.M.’s Department. M.G.M. is a member of the IV Fluids Guideline Development Group for the National Institute of Clinical Excellence (NICE) and he is a co-author of the GIFTASUP fluid guidelines. A.S. received grant support from Baxter Healthcare related to Plasmalyte, and serves as a paid consultant for Baxter and Grifols. K.M., J.L., and D.Y. have none to declare.
Figures
References
-
- Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345:1368–77. - PubMed
-
- Brunkhorst FM, Engel C, Bloos F, et al. Intensive insulin therapy and pentastarch resuscitation in severe sepsis. N Engl J Med. 2008;358:125–39. - PubMed
-
- Shaw AD, Bagshaw SM, Goldstein SL, et al. Major complications, mortality, and resource utilization after open abdominal surgery: 0.9% saline compared to Plasma-Lyte. Ann Surg. 2012;255:821–9. - PubMed
-
- Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney injury in critically ill adults. J Am Med Assoc. 2012;308:1566–72. - PubMed
-
- Perner A, Haase N, Guttormsen AB, et al. Hydroxyethyl starch 130/0.4 versus Ringer’s acetate in severe sepsis. N Engl J Med. 2012;367:124–34. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
