

Variability in MRI vs. ultrasound measures of prostate volume and its impact on treatment recommendations for favorable-risk prostate cancer patients: a case series
- PMID: 25205146
- PMCID: PMC4261899
- DOI: 10.1186/1748-717X-9-200
Variability in MRI vs. ultrasound measures of prostate volume and its impact on treatment recommendations for favorable-risk prostate cancer patients: a case series
Abstract
Background: Prostate volume can affect whether patients qualify for brachytherapy (desired size ≥20 mL and ≤60 mL) and/or active surveillance (desired PSA density ≤0.15 for very low risk disease). This study examines variability in prostate volume measurements depending on imaging modality used (ultrasound versus MRI) and volume calculation technique (contouring versus ellipsoid) and quantifies the impact of this variability on treatment recommendations for men with favorable-risk prostate cancer.
Methods: We examined 70 patients who presented consecutively for consideration of brachytherapy for favorable-risk prostate cancer who had volume estimates by three methods: contoured axial ultrasound slices, ultrasound ellipsoid (height × width × length × 0.523) calculation, and endorectal coil MRI (erMRI) ellipsoid calculation.
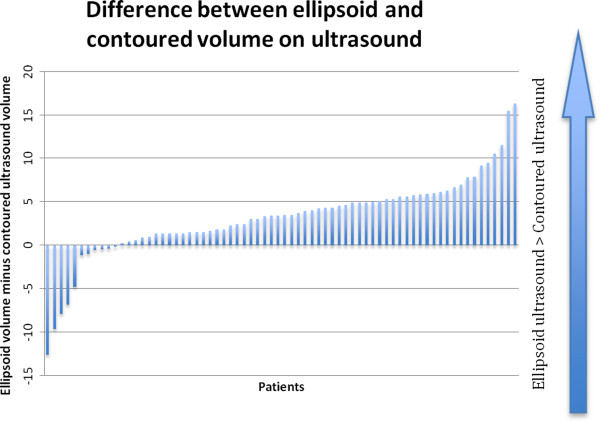
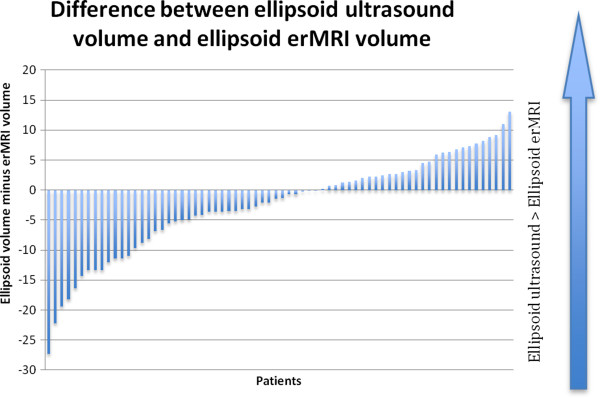
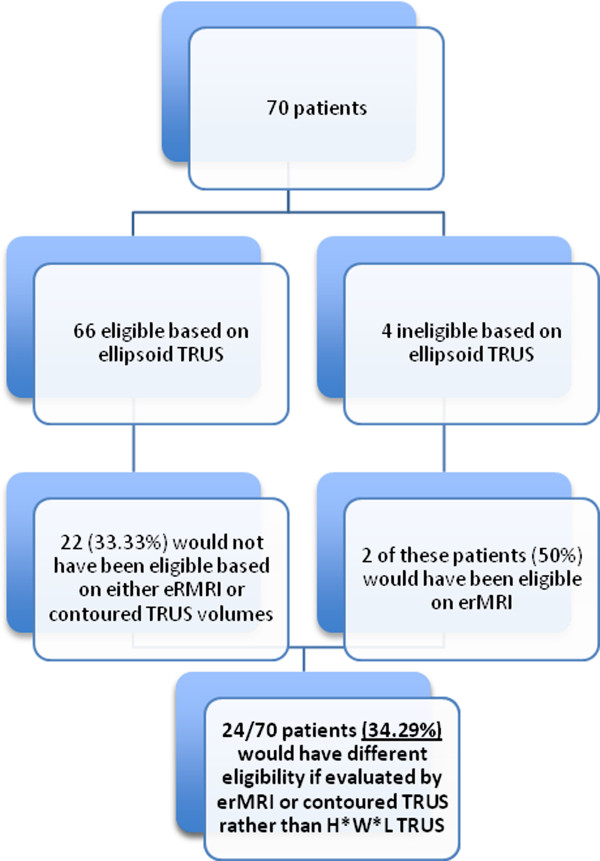
Results: Average gland size by the contoured ultrasound, ellipsoid ultrasound, and erMRI methods were 33.99, 37.16, and 39.62 mLs, respectively. All pairwise comparisons between methods were statistically significant (all p < 0.015). Of the 66 patients who volumetrically qualified for brachytherapy on ellipsoid ultrasound measures, 22 (33.33%) did not qualify on ellipsoid erMRI or contoured ultrasound measures. 38 patients (54.28%) had PSA density ≤0.15 ng/dl as calculated using ellipsoid ultrasound volumes, compared to 34 (48.57%) and 38 patients (54.28%) using contoured ultrasound and ellipsoid erMRI volumes, respectively.
Conclusions: The ultrasound ellipsoid and erMRI ellipsoid methods appeared to overestimate ultrasound contoured volume by an average of 9.34% and 16.57% respectively. 33.33% of those who qualified for brachytherapy based on ellipsoid ultrasound volume would be disqualified based on ultrasound contoured and/or erMRI ellipsoid volume. As treatment recommendations increasingly rely on estimates of prostate size, clinicians must consider method of volume estimation.
Figures
References
-
- Davis BJ, Horwitz EM, Lee WR, Crook JM, Stock RG, Merrick GS, Butler WM, Grimm PD, Stone NN, Potters L, Zietman AL, Zelefsky MJ, American Brachytherapy Society American Brachytherapy Society consensus guidelines for transrectal ultrasound-guided permanent prostate brachytherapy. Brachytherapy. 2012;11:6–19. doi: 10.1016/j.brachy.2011.07.005. - DOI - PubMed
-
- Mohler JL, Kantoff PW, Armstrong AJ, Bahnson RR, Cohen M, D’Amico AV, Eastham JA, Enke CA, Farrington TA, Higano CS, Horwitz EM, Kane CJ, Kawachi MH, Kuettel M, Kuzel TM, Lee RJ, Malcom AW, Miller D, Pilmack ER, Pow-Sang JM, Raben D, Richey S, Roach M, 3rd, Rohren E, Rosenfeld S, Schaeffer E, Small EJ, Sonpavde G, Srinivas S, Stein C, et al. Prostate cancer, version 2.2014. J Natl Compr Canc Netw. 2014;12:686–718. - PubMed
-
- Loblaw DA, Wallner K, Dibiase S, Russell K, Blasko J, Ellis W. Brachytherapy in patients with small prostate glands. Tech Urol. 2000;6:64–69. - PubMed
-
- Merrick GS, Butler WM, Dorsey AT, Lief JH. Effect of prostate size and isotope selection on dosimetric quality following permanent seed implantation. Tech Urol. 2001;7:233–240. - PubMed
-
- Nguyen PL, Chen MH, Choueiri TK, Hoffman KE, Hu JC, Martin NE, Beard CJ, Dosoretz DE, Moran BJ, Katin MJ, Braccioforte MH, Ross R, Salenius SA, Kantoff PW, D’Amico AV. Risk of all-cause and prostate-specific mortality after brachytherapy in men with small prostate size? Int J Radiat Oncol Biol Phys. 2011;79:1318–1322. doi: 10.1016/j.ijrobp.2010.01.023. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
