

A dosimetric comparison of three-dimensional conformal radiotherapy, volumetric-modulated arc therapy, and dynamic conformal arc therapy in the treatment of non-small cell lung cancer using stereotactic body radiotherapy
- PMID: 25207575
- PMCID: PMC5711086
- DOI: 10.1120/jacmp.v15i5.4898
A dosimetric comparison of three-dimensional conformal radiotherapy, volumetric-modulated arc therapy, and dynamic conformal arc therapy in the treatment of non-small cell lung cancer using stereotactic body radiotherapy
Abstract
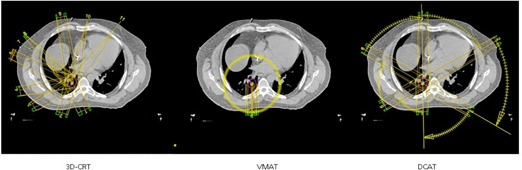
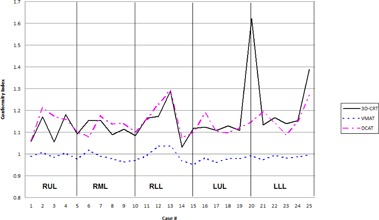
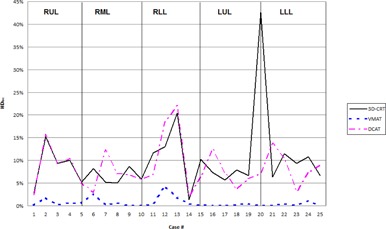
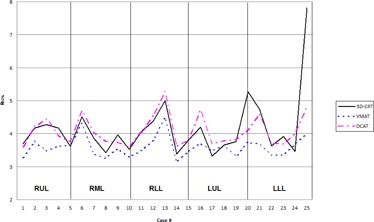
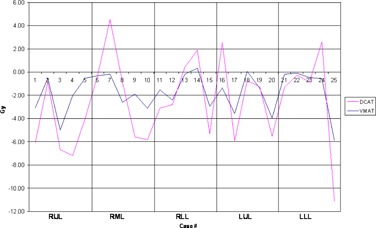
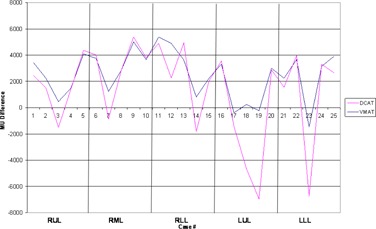
This study evaluates three-dimensional conformal radiotherapy (3D CRT), volumetric-modulated arc therapy (VMAT), and dynamic conformal arc therapy (DCAT) planning techniques using dosimetric indices from Radiation Therapy Oncology Group (RTOG) protocols 0236, 0813, and 0915 for the treatment of early-stage non-small cell lung cancer (NSCLC) using stereotactic body radiotherapy (SBRT). Twenty-five clinical patients, five per lung lobe, previously treated for NSCLC using 3D CRT SBRT under respective RTOG protocols were replanned with VMAT and DCAT techniques. All plans were compared using respective RTOG dosimetric indices. High- and low-dose spillage improved for VMAT and DCAT plans, though only VMAT was able to improve dose to all organs at risk (OARs). DCAT was only able to provide a minimal improvement in dose to the heart and ipsilateral brachial plexus. Mean bilateral, contralateral, and V20 (percentage of bilateral lung receiving at least 20 Gy dose) doses were reduced with VMAT in comparison with respective 3D CRT clinical plans. Though some of the DCAT plans had values for the above indices slightly higher than their respective 3D CRT plans, they still were able to meet the RTOG constraints. VMAT and DCAT were able to offer improved skin dose by 1.1% and 11%, respectively. Monitor units required for treatment delivery increased with VMAT by 41%, but decreased with DCAT by 26%. VMAT and DCAT provided improved dose distributions to the PTV, but only VMAT was consistently superior in sparing dose to OARs in all the five lobes. DCAT should still remain an alternative to 3D CRT in facilities that do not have VMAT or intensity-modulated radiotherapy (IMRT) capabilities.
Figures
References
-
- Timmerman R, McGarry R, Yiannoutsos C et al. Excessive toxicity when treating central tumors in a phase II study of stereotactic body radiation therapy for medically inoperable early‐stage lung cancer. J Clin Oncol. 2006;24(30)4833–39. - PubMed
-
- Xia T, Li H, Sun Q et al. Promising clinical outcome of stereotactic body radiation therapy for patients with inoperable Stage I/II non‐small‐cell lung cancer. Int J Radiat Oncol Biol Phys. 2006;66(1):117–25. - PubMed
-
- Baumann P, Nyman J, Hoyer M et al. Outcome in a prospective phase II trial of medically inoperable stage I non‐small‐cell lung cancer patients treated with stereotactic body radiotherapy. J Clin Oncol. 2009;27(20):3290–96. - PubMed
-
- McGrath SD, Matuszak MM, Yan D, Kastin LL, Martinez AA, Grills IS. Volumetric modulated arc therapy for delivery of hypofractionated stereotactic lung radiotherapy: A dosimetric and treatment efficiency analysis. Radiother Oncol. 2010;95(2):153–57. - PubMed
-
- Lee TF, Chao PJ, Wang CY et al. Dosimetric comparison of helical tomotherapy and dynamic conformal arc therapy in stereotactic radiosurgery for vestibular schwannomas. Med Dosim. 2011;36(1):62–70. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
