

Direct traumatic carotid cavernous fistula: angiographic classification and treatment strategies. Study of 172 cases
- PMID: 25207910
- PMCID: PMC4187443
- DOI: 10.15274/INR-2014-10020
Direct traumatic carotid cavernous fistula: angiographic classification and treatment strategies. Study of 172 cases
Abstract
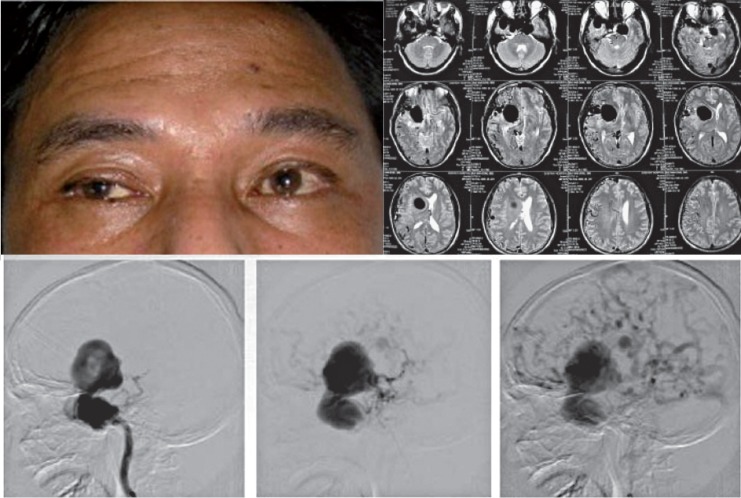
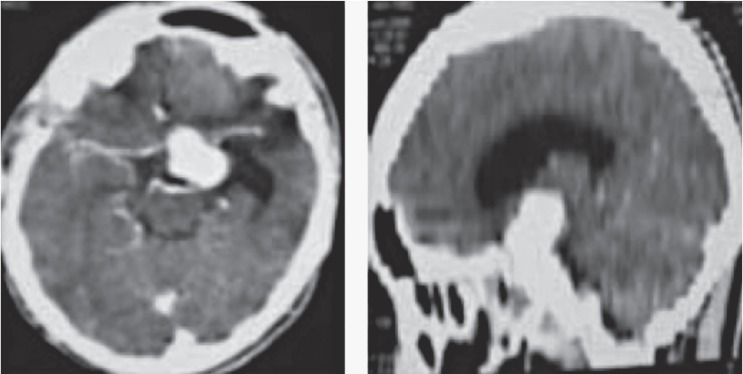
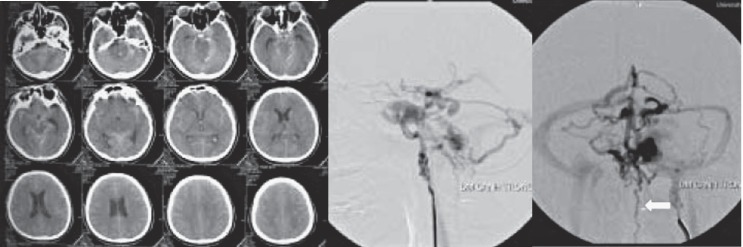
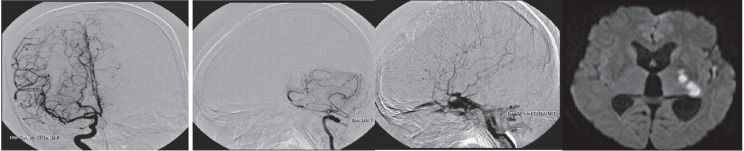
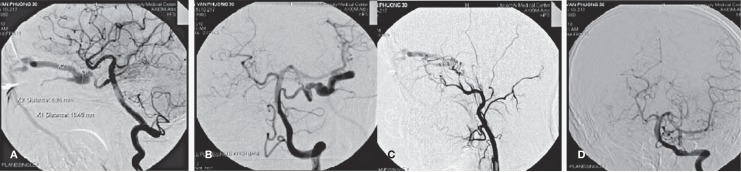
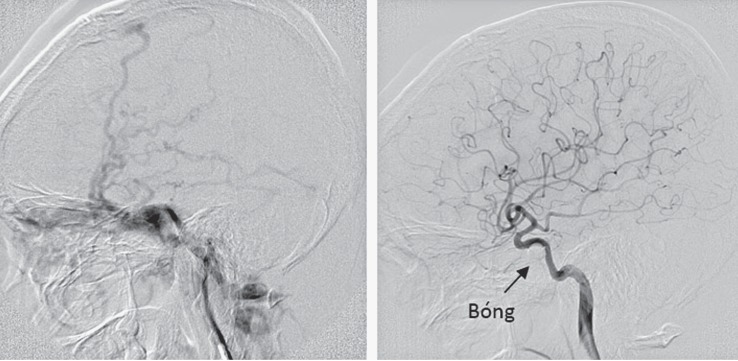
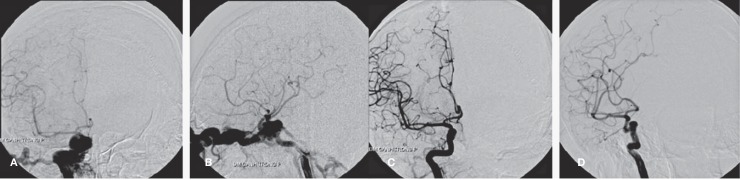
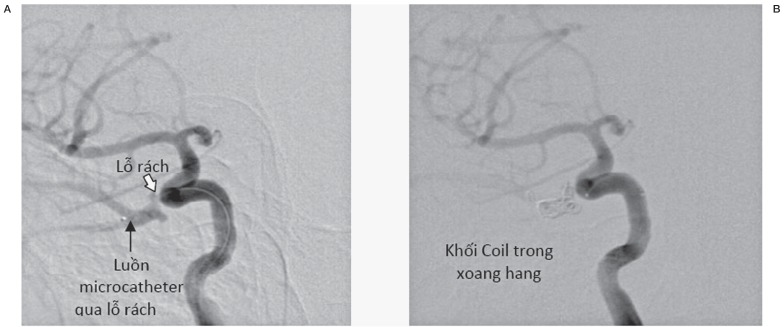
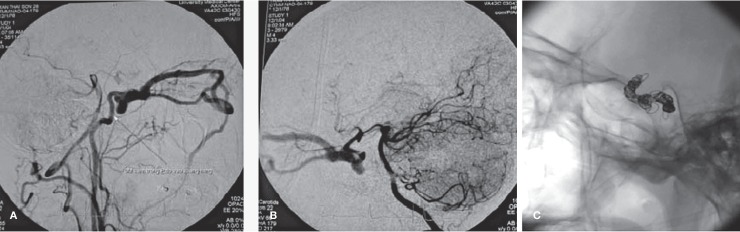
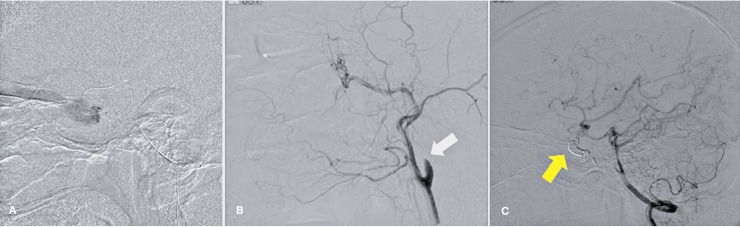
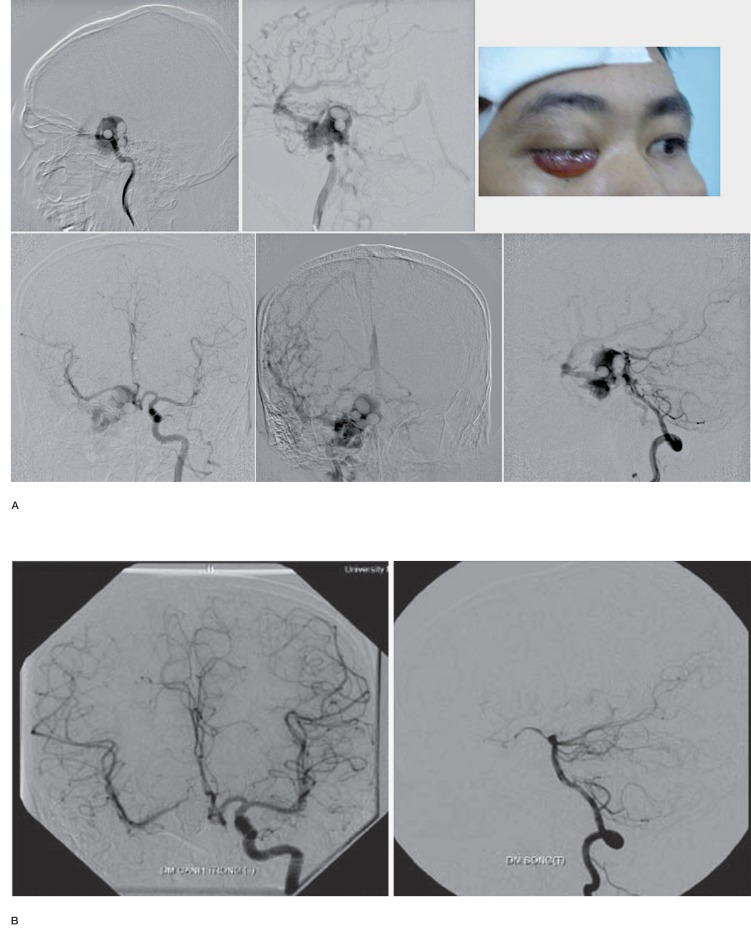
We report our experience in treatment of traumatic direct carotid cavernous fistula (CCF) via endovascular intervention. We hereof recommend an additional classification system for type A CCF and suggest respective treatment strategies. Only type A CCF patients (Barrow's classification) would be recruited for the study. Based on the angiographic characteristics of the CCF, we classified type A CCF into three subtypes including small size, medium size and large size fistula depending on whether there was presence of the anterior carotid artery (ACA) and/or middle carotid artery (MCA). Angiograms with opacification of both ACA and MCA were categorized as small size fistula. Angiograms with opacification of either ACA or MCA were categorized as medium size fistula and those without opacification of neither ACA nor MCA were classified as large size fiatula. After the confirm angiogram, endovascular embolization would be performed impromptu using detachable balloon, coils or both. All cases were followed up for complication and effect after the embolization. A total of 172 direct traumatic CCF patients were enrolled. The small size fistula was accountant for 12.8% (22 cases), medium size 35.5% (61 cases) and large size fistula accountant for 51.7% (89 cases). The successful rate of fistula occlusion under endovascular embolization was 94% with preservation of the carotid artery in 70%. For the treatment of each subtype, a total of 21/22 cases of the small size fistulas were successfully treated using coils alone. The other single case of small fistula was defaulted. Most of the medium and large size fistulas were cured using detachable balloons. When the fistula sealing could not be obtained using detachable balloon, coils were added to affirm the embolization of the cavernous sinus via venous access. There were about 2.9% of patient experienced direct carotid artery puncture and 0.6% puncture after carotid artery cut-down exposure. About 30% of cases experienced sacrifice of the parent vessels and it was associated with sizes of the fistula. Total severe complication was about 2.4% which included 1 death (0.6%) due to vagal shock; 1 transient hemiparesis post-sacrifice occlusion of the carotid artery but the patient had recovered after 3 months; 1 acute thrombus embolism and the patient was completely saved with recombinant tissue plaminogen activator (rTPA); 1 balloon dislodgement then got stuck at the anterior communicating artery but the patient was asymptomatic. Endovascular intervention as the treatment of direct traumatic CCF had high cure rate and low complication with its ability to preserve the carotid artery. It also can supply flexible accesses to the fistulous site with various alternative embolic materials. The new classification of type A CCF based on angiographic features was helpful for planning for the embolization. Coil should be considered as the first embolic material for small size fistula meanwhile detachable balloons was suggested as the first-choice embolic agent for the medium and large size fistula.
Keywords: carotid cavernous fistula; contralateral internal carotid artery approach; internal carotid artery ligation; percutaneous cavernous sinus embolization.
Figures

Similar articles
-
Recurrent carotico-cavernous fistula after internal carotid artery ligation: a case with embolization of the fistula via contralateral internal carotid artery approach.Interv Neuroradiol. 2014 Jul-Aug;20(4):482-6. doi: 10.15274/INR-2014-10021. Epub 2014 Aug 28. Interv Neuroradiol. 2014. PMID: 25207912 Free PMC article.
-
Embolization of direct carotid cavernous fistulas with the novel double-balloon technique.Interv Neuroradiol. 2016 Apr;22(2):201-5. doi: 10.1177/1591019915609779. Epub 2015 Nov 18. Interv Neuroradiol. 2016. PMID: 26586136 Free PMC article.
-
The evolution of endovascular treatment of carotid cavernous fistulas: a single-center experience.World Neurosurg. 2013 Nov;80(5):538-48. doi: 10.1016/j.wneu.2013.02.033. Epub 2013 Feb 9. World Neurosurg. 2013. PMID: 23402868
-
Direct Carotid Cavernous Fistulas.J Neuroendovasc Ther. 2020;14(12):583-592. doi: 10.5797/jnet.ra.2020-0131. Epub 2020 Nov 25. J Neuroendovasc Ther. 2020. PMID: 37502141 Free PMC article. Review.
-
Transvenous approach for the treatment of direct carotid cavernous fistula following Pipeline embolization of cavernous carotid aneurysm: a report of two cases and review of the literature.J Neurointerv Surg. 2015 Aug;7(8):e30. doi: 10.1136/neurintsurg-2014-011235.rep. Epub 2014 Aug 1. J Neurointerv Surg. 2015. PMID: 25085458 Review.
Cited by
-
Direct carotid-cavernous fistulas occurring during neurointerventional procedures.Interv Neuroradiol. 2016 Feb;22(1):91-6. doi: 10.1177/1591019915617321. Epub 2015 Nov 30. Interv Neuroradiol. 2016. PMID: 26628454 Free PMC article.
-
Connecting the dots: Linking superior ophthalmic vein and internal jugular vein diameter to carotid cavernous fistula type and location.Surg Neurol Int. 2024 Oct 18;15:377. doi: 10.25259/SNI_601_2024. eCollection 2024. Surg Neurol Int. 2024. PMID: 39524569 Free PMC article.
-
Dissection-related carotid-cavernous fistula (CCF) following surgical revascularization of chronic internal carotid artery occlusion: a new subtype of CCF and proposed management.Chin Neurosurg J. 2020 Jan 10;6:2. doi: 10.1186/s41016-019-0180-9. eCollection 2020. Chin Neurosurg J. 2020. PMID: 32922931 Free PMC article.
-
Usefulness of Stent-Assisted Coil Embolization of Direct Traumatic Carotid-Cavernous Fistulas: Report of Three Patients and Review of Other Treatment Methods.J Neuroendovasc Ther. 2020;14(11):514-521. doi: 10.5797/jnet.tn.2020-0031. Epub 2020 Aug 28. J Neuroendovasc Ther. 2020. PMID: 37501769 Free PMC article.
-
Direct Carotid-Cavernous Fistula due to Aneurysmal Rupture with Residual Aortic Dissection Treated by Coil Embolization via Direct Puncture of the Common Carotid Artery: A Case Report.J Neuroendovasc Ther. 2025;19(1):2025-0061. doi: 10.5797/jnet.cr.2025-0061. Epub 2025 Aug 1. J Neuroendovasc Ther. 2025. PMID: 40761444 Free PMC article.
References
-
- Barrow DL, Spector RH, Braun IF, et al. Classification and treatment of spontaneous carotid-cavernous sinus fistulas. J Neurosurg. 1985;62(2):248–256. doi: 10.3171/jns.1985.62.2.0248. - DOI - PubMed
-
- Lewis AI, Tomsick TA, Tew JM., Jr Management of 100 consecutive direct carotid-cavernous fistulas: results of treatment with detachable balloons. Neurosurgery. 1995;36(2):239–244. doi: 10.1227/00006123-199502000-00001. - DOI - PubMed
-
- Guglielmi G, Viñuela F, Briganti F, et al. Carotid-cavernous fistula caused by a ruptured intracavernous aneurysm: endovascular treatment by electrothrombosis with detachable coils. Neurosurgery. 1992;31(3):591–596. doi: 10.1227/00006123-199209000-00026. - DOI - PubMed
-
- Brooks B. The Treatment of Traumatic Arteriovenous Fistula. Southern Medical Journal. 1930;23(2):100–106. doi: 10.1097/00007611-193002000-00004. - DOI
-
- Parkinson D. Carotid cavernous fistula: direct repair with preservation of the carotid artery. Technical note. J Neurosurg. 1973;38(1):99–106. doi: 10.3171/jns.1973.38.1.0099. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
