

Higher risk of death and stroke in patients with persistent vs. paroxysmal atrial fibrillation: results from the ROCKET-AF Trial
- PMID: 25209598
- PMCID: PMC4313363
- DOI: 10.1093/eurheartj/ehu359
Higher risk of death and stroke in patients with persistent vs. paroxysmal atrial fibrillation: results from the ROCKET-AF Trial
Abstract
Aim: Anticoagulation prophylaxis for stroke is recommended for at-risk patients with either persistent or paroxysmal atrial fibrillation (AF). We compared outcomes in patients with persistent vs. paroxysmal AF receiving oral anticoagulation.
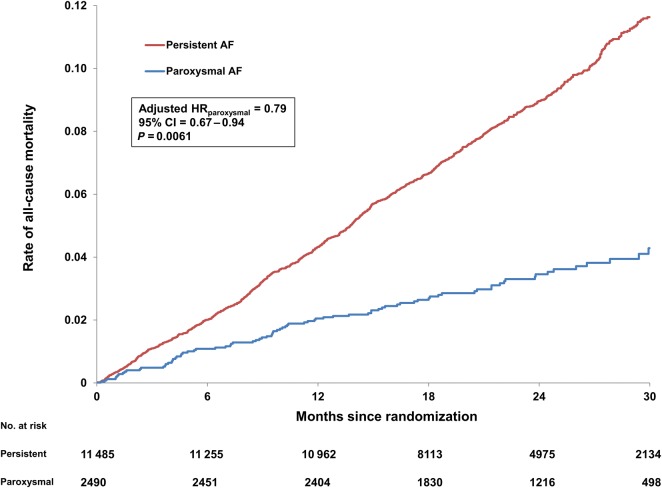
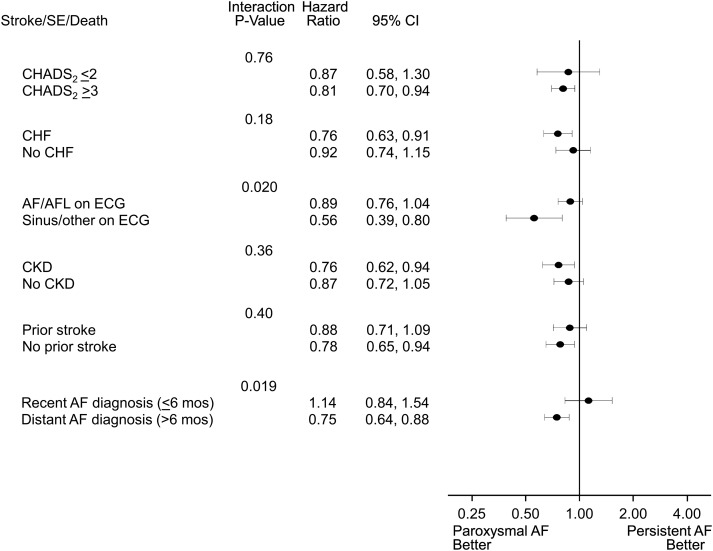
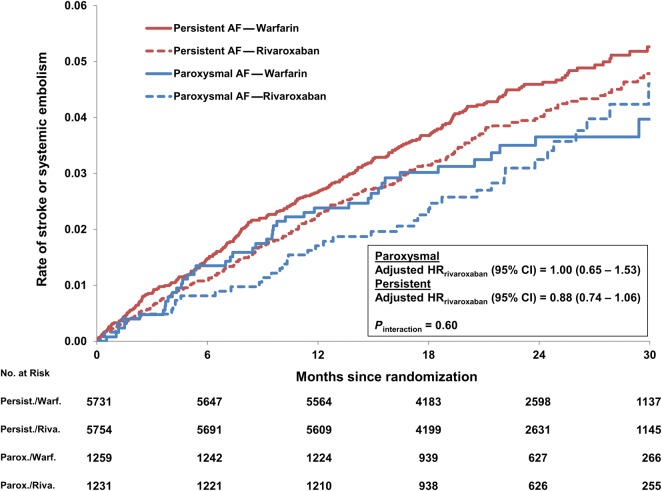
Methods and results: Patients randomized in the Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared With Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET-AF) trial (n = 14 264) were grouped by baseline AF category: paroxysmal or persistent. Multivariable adjustment was performed to compare thrombo-embolic events, bleeding, and death between groups, in high-risk subgroups, and across treatment assignment (rivaroxaban or warfarin). Of 14 062 patients, 11 548 (82%) had persistent AF and 2514 (18%) had paroxysmal AF. Patients with persistent AF were marginally older (73 vs. 72, P = 0.03), less likely female (39 vs. 45%, P < 0.0001), and more likely to have previously used vitamin K antagonists (64 vs. 56%, P < 0.0001) compared with patients with paroxysmal AF. In patients randomized to warfarin, time in therapeutic range was similar (58 vs. 57%, P = 0.94). Patients with persistent AF had higher adjusted rates of stroke or systemic embolism (2.18 vs. 1.73 events per 100-patient-years, P = 0.048) and all-cause mortality (4.78 vs. 3.52, P = 0.006). Rates of major bleeding were similar (3.55 vs. 3.31, P = 0.77). Rates of stroke or systemic embolism in both types of AF did not differ by treatment assignment (rivaroxaban vs. warfarin, Pinteraction = 0.6).
Conclusion: In patients with AF at moderate-to-high risk of stroke receiving anticoagulation, those with persistent AF have a higher risk of thrombo-embolic events and worse survival compared with paroxysmal AF.
Keywords: Anticoagulation; Atrial fibrillation; Outcomes; Paroxysmal; Persistent.
© The Author 2014. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
References
-
- Suzuki T, Yamazaki T, Ogawa S, Nagai R, Yamashita T. Echocardiographic predictors of frequency of paroxysmal atrial fibrillation (AF) and its progression to persistent AF in hypertensive patients with paroxysmal AF: Results from the Japanese Rhythm Management Trial II for Atrial Fibrillation (J-RHYTHM II Study) Heart Rhythm. 2011;8:1831–1836. - PubMed
-
- Chiang CE, Naditch-Brule L, Murin J, Goethals M, Inoue H, O'Neill J, Silva-Cardoso J, Zharinov O, Gamra H, Alam S, Ponikowski P, Lewalter T, Rosenqvist M, Steg PG. Distribution and risk profile of paroxysmal, persistent, and permanent atrial fibrillation in routine clinical practice: insight from the real-life global survey evaluating patients with atrial fibrillation international registry. Circ Arrhythm Electrophysiol. 2012;5:632–639. - PubMed
-
- Wilber DJ, Pappone C, Neuzil P, De Paola A, Marchlinski F, Natale A, Macle L, Daoud EG, Calkins H, Hall B, Reddy V, Augello G, Reynolds MR, Vinekar C, Liu CY, Berry SM, Berry DA, ThermoCool AFTI. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010;303:333–340. - PubMed
-
- Camm AJ, Kirchhof P, Lip GY, Schotten U, Savelieva I, Ernst S, Van Gelder IC, Al-Attar N, Hindricks G, Prendergast B, Heidbuchel H, Alfieri O, Angelini A, Atar D, Colonna P, De Caterina R, De Sutter J, Goette A, Gorenek B, Heldal M, Hohloser SH, Kolh P, Le Heuzey JY, Ponikowski P, Rutten FH. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC) Eur Heart J. 2010;31:2369–2429. - PubMed
-
- Singer DE, Albers GW, Dalen JE, Fang MC, Go AS, Halperin JL, Lip GY, Manning WJ. Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition) Chest. 2008;133(6 Suppl):546S–592S. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
