

Cerebellar haemorrhage mimicking acute peripheral vestibulopathy: the role of the video head impulse test in differential diagnosis
- PMID: 25210225
- PMCID: PMC4157530
Cerebellar haemorrhage mimicking acute peripheral vestibulopathy: the role of the video head impulse test in differential diagnosis
Abstract
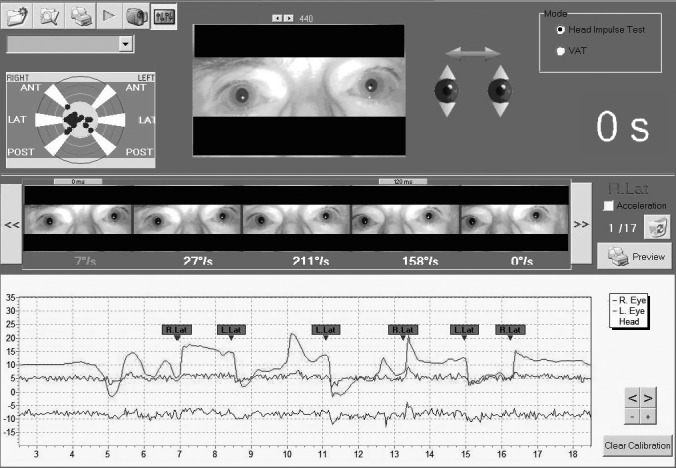
Dizziness and vertigo without neurological signs are typically due to a peripheral vestibular disease. Although the most common causes are benign, differential diagnosis must include potentially life-threatening central diseases such as cerebrovascular pathologies. A systemic clinical approach needs a careful work-up, bedside examination and appropriate instrumental investigation. The head impulse test (HIT) allows qualitative clinical assessment of canalar function; it has some limitations such as subjective evaluation, mainly in patients with a spontaneous nystagmus. A new device has been recently developed consisting of an infrared video camera (video-HIT) to provide quantitative instrumental assessment of the high-frequency vestibular-ocular reflex (VOR) gain. By reporting a case of cerebellar haemorrhage mimicking an acute peripheral vestibulopathy, the authors suggest that video-HIT may be considered a useful tool in differential diagnosis between vestibular neuritis and cerebellar vascular disease in patients with severe acute vertigo without central signs.
Una sindrome vertiginosa non associata a segni clinici neurologici è più comunemente è riferibile ad una patologia vestibolare periferica. Anche se le cause più comuni sono benigne, la diagnosi differenziale deve includere le malattie centrali potenzialmente letali come quelle cerebrovascolari. Un approccio sistemico necessita di un'attenta anamnesi, di un esame clinico e di un'appropriata indagine strumentale. Il test impulsivo rotatorio o head impulse test (HIT) permette una valutazione qualitativa clinica della funzione canalare ma presenta alcuni limiti legati soprattutto alla valutazione soggettiva, specialmente in pazienti con nistagmo spontaneo. Un nuovo dispositivo, che utilizza una telecamera ad infrarossi video (video-HIT), è stato sviluppato di recente per fornire una valutazione quantitativa strumentale del guadagno del riflesso vestibulo-oculare (VOR) ad alta frequenza. Descrivendo il caso clinico di un'emorragia cerebellare che potrebbe simulare una vestibulopatia periferica acuta, gli autori dimostrano che il video-HIT può essere uno strumento molto utile nella diagnosi differenziale tra neurite vestibolare e malattia vascolare cerebellare in pazienti con vertigine severa acuta senza segni centrali.
Keywords: Central vertigo; Cerebellar haemorrhage; Head impulse test; Peripheral vertigo; Vestibular neuritis.
Figures



Similar articles
-
VOR gain by head impulse video-oculography differentiates acute vestibular neuritis from stroke.Otol Neurotol. 2015 Mar;36(3):457-65. doi: 10.1097/MAO.0000000000000638. Otol Neurotol. 2015. PMID: 25321888
-
Normal head impulse test differentiates acute cerebellar strokes from vestibular neuritis.Neurology. 2008 Jun 10;70(24 Pt 2):2378-85. doi: 10.1212/01.wnl.0000314685.01433.0d. Neurology. 2008. PMID: 18541870
-
Acute unilateral vestibulopathy/vestibular neuritis: Diagnostic criteria.J Vestib Res. 2022;32(5):389-406. doi: 10.3233/VES-220201. J Vestib Res. 2022. PMID: 35723133 Free PMC article.
-
Use of HINTS in the acute vestibular syndrome. An Overview.Stroke Vasc Neurol. 2018 Jun 23;3(4):190-196. doi: 10.1136/svn-2018-000160. eCollection 2018 Dec. Stroke Vasc Neurol. 2018. PMID: 30637123 Free PMC article. Review.
-
Acute Vestibular Syndrome.Continuum (Minneap Minn). 2021 Apr 1;27(2):402-419. doi: 10.1212/CON.0000000000000958. Continuum (Minneap Minn). 2021. PMID: 34351112 Review.
Cited by
-
Stroke prediction in patients presenting with isolated dizziness in the emergency department.Sci Rep. 2021 Mar 17;11(1):6114. doi: 10.1038/s41598-021-85725-1. Sci Rep. 2021. PMID: 33731825 Free PMC article.
-
R-cVR, a two-step bedside algorithm for the differential diagnosis of acute dizziness and vertigo.Heliyon. 2024 Sep 26;10(19):e38532. doi: 10.1016/j.heliyon.2024.e38532. eCollection 2024 Oct 15. Heliyon. 2024. PMID: 39397912 Free PMC article.
-
Diagnosis of benign paroxysmal positional vertigo in Emergency Department: Our experience.Audiol Res. 2020 Jul 10;10(1):232. doi: 10.4081/audiores.2020.232. eCollection 2020 Jul 7. Audiol Res. 2020. PMID: 32774823 Free PMC article.
-
STANDING, a four-step bedside algorithm for differential diagnosis of acute vertigo in the Emergency Department.Acta Otorhinolaryngol Ital. 2014 Dec;34(6):419-26. Acta Otorhinolaryngol Ital. 2014. PMID: 25762835 Free PMC article.
-
[Video head impulse test for evaluation of vestibular function in patients with vestibular neuritis and benign paroxysmal positional vertigo].Zhejiang Da Xue Xue Bao Yi Xue Ban. 2017 Jan 25;46(1):52-58. doi: 10.3785/j.issn.1008-9292.2017.02.08. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2017. PMID: 28436631 Free PMC article. Chinese.
References
-
- Gomez CR, Cruz-Flores S, Malkoff MD, et al. Isolated vertigo as a manifestation of vertebrobasilar ischemia. Neurology. 1996;47:94–97. - PubMed
-
- Lee H, Cho YW. A case of isolated nodulus infarction presenting as a vestibular neuritis. J Neurol Sci. 2004;221:117–119. - PubMed
-
- Kim HA, Lee SR, Lee H. Acute peripheral vestibular syndrome of a vascular cause. J Neurol Sci. 2007;254:99–101. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources