

Basilar invagination: Surgical results
- PMID: 25210337
- PMCID: PMC4158635
- DOI: 10.4103/0974-8237.139202
Basilar invagination: Surgical results
Abstract
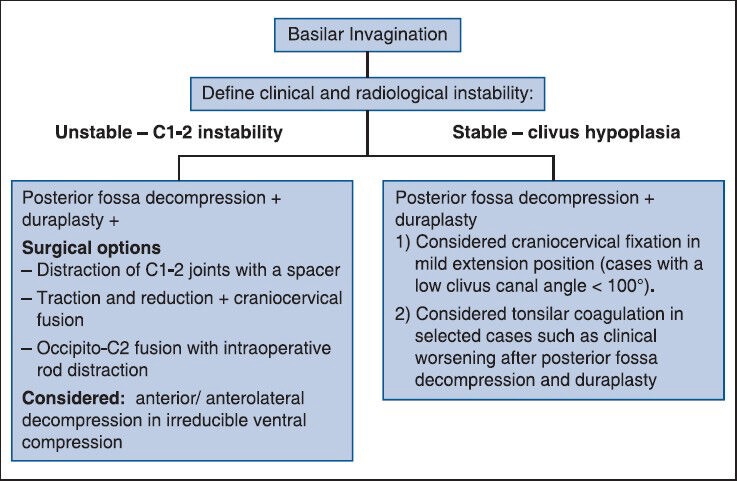
Introduction: Basilar invagination (BI) is a congenital craniocervical junction (CCJ) anomaly represented by a prolapsed spine into the skull-base that can result in severe neurological impairment.
Materials and methods: In this paper, we retrospective evaluate the surgical treatment of 26 patients surgically treated for symptomatic BI. BI was classified according to instability and neural abnormalities findings. Clinical outcome was evaluated using the Nürick grade system.
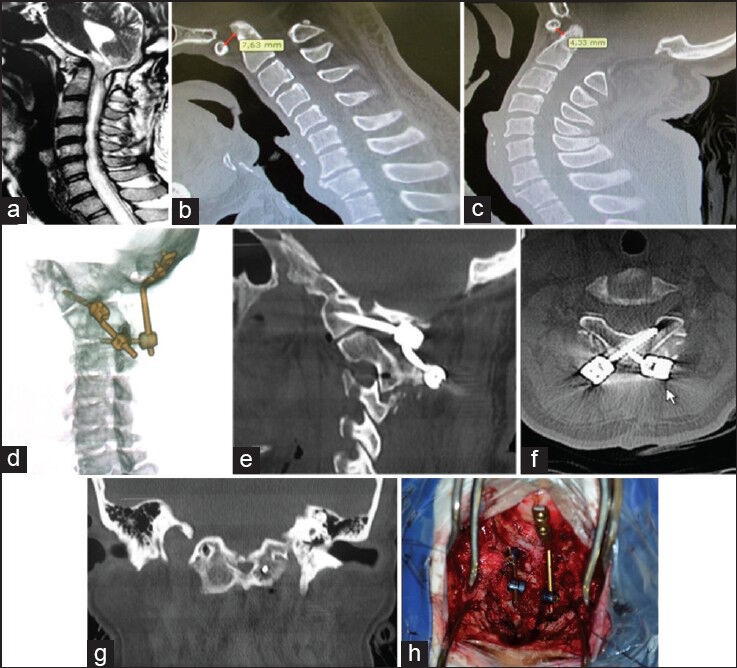
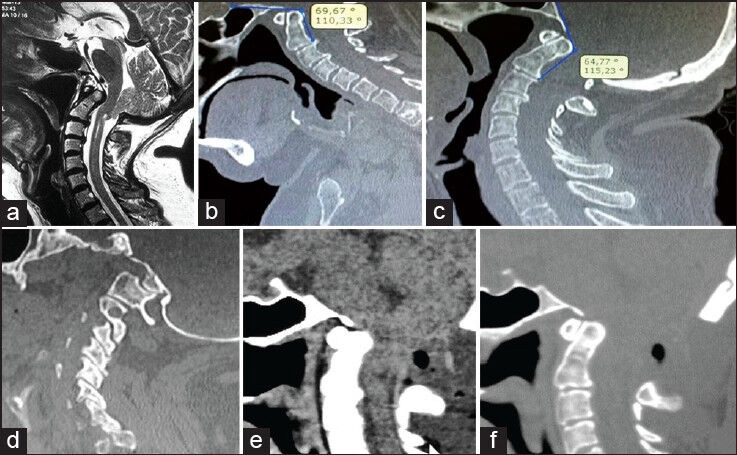
Results: A total of 26 patients were included in this paper. Their age ranged from 15 to 67 years old (mean 38). Of which, 10 patients were male (38%) and 16 (62%) were female. All patients had some degree of tonsillar herniation, with 25 patients treated with foramen magnum decompression. Nine patients required a craniocervical fixation. Six patients had undergone prior surgery and required a new surgical procedure for progression of neurological symptoms associated with new compression or instability. Most of patients with neurological symptoms secondary to brainstem compression had some improvement during the follow-up. There was mortality in this series, 1 month after surgery, associated with a late removal of the tracheal cannula.
Conclusions: Management of BI requires can provide improvements in neurological outcomes, but requires analysis of the neural and bony anatomy of the CCJ, as well as occult instability. The complexity and heterogeneous presentation requires attention to occult instability on examination and attention to airway problems secondary to concomitant facial malformations.
Keywords: Basilar invagination; congenital craniocervical malformation; surgical treatment.
Conflict of interest statement
Figures
References
-
- Dickman CA, Lekovic GP. Biomechanical considerations for stabilization of the craniovertebral junction. Clin Neurosurg. 2005;52:205–13. - PubMed
-
- Joaquim AF, Ghizoni E, Rubino PA, Anderle DV, Tedeschi H, Rhoton AL, Jr, et al. Lateral mass screw fixation of the atlas: Surgical technique and anatomy. World Neurosurg. 2010;74:359–62. - PubMed
-
- Joaquim AF, Cavalcante RA, Rodrigues IJ, Mudo ML. Occipito-C2 laminar screws fixation for treatment of chronic C1-2 instability. J Bras Neurocirugía. 2011;22:186–9.
-
- Joaquim AF, Patel AP. Occipito cervical trauma: Evaluation, classification and treatment. Contemp Spine Surg. 2010;11:1–5.
-
- Joaquim AF, Patel AP. C1 and C2 spine trauma: Evaluation, classification and treatment. Contemp Spine Surg. 2010;11:1–7.
LinkOut - more resources
Full Text Sources
Other Literature Sources
