

Correction of metopic synostosis utilizing an in situ bandeau approach
- PMID: 25210504
- PMCID: PMC4154973
- DOI: 10.1055/s-0034-1384806
Correction of metopic synostosis utilizing an in situ bandeau approach
Abstract
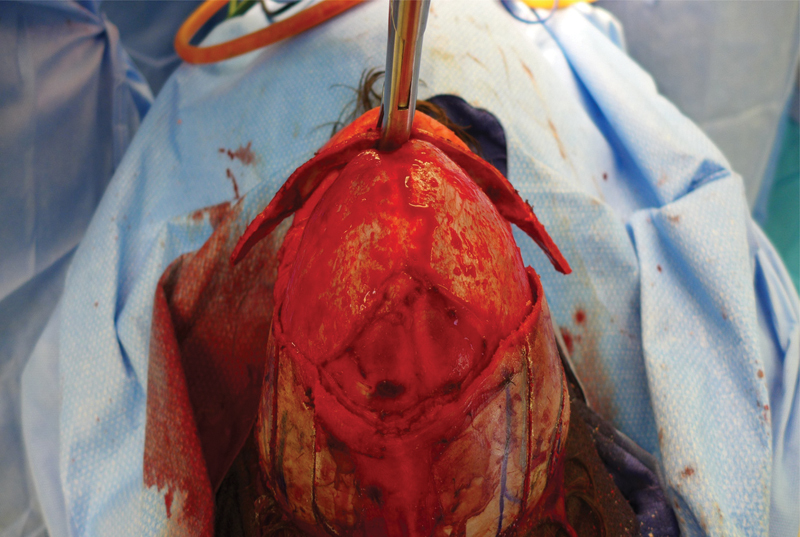
Metopic craniosynostosis is a common growth disturbance in the infant cranium, second only to sagittal synostosis. Presenting symptoms are usually of a clinical nature and are defined by an angular forehead, retruded lateral brow, bitemporal narrowing, and a broad-based occiput. These changes create the pathognomonic trigonocephalic cranial shape. Aesthetic in nature, these morphological changes do not constitute the only developmental issues faced by children who present with this malady. Recent studies and anecdotal evidence have also demonstrated that children who present with metopic synostosis may face issues with respect to intellectual and/or psychological development. The authors present an elegant approach to the surgical reconstruction of the trigonocephalic cranium using an in situ bandeau approach.
Keywords: craniosynostosis; metopic; suture; trigonocephaly.
Figures







Similar articles
-
Little evidence of association between severity of trigonocephaly and cognitive development in infants with single-suture metopic synostosis.Neurosurgery. 2010 Aug;67(2):408-15; discussion 415-6. doi: 10.1227/01.NEU.0000371992.72539.8B. Neurosurgery. 2010. PMID: 20644427 Free PMC article.
-
Trigonocephaly: Long-term results after surgical correction of metopic suture synostosis.Adv Clin Exp Med. 2019 May;28(5):625-635. doi: 10.17219/acem/90763. Adv Clin Exp Med. 2019. PMID: 30712337
-
Structural brain differences in school-age children with and without single-suture craniosynostosis.J Neurosurg Pediatr. 2017 Apr;19(4):479-489. doi: 10.3171/2016.9.PEDS16107. Epub 2017 Feb 3. J Neurosurg Pediatr. 2017. PMID: 28156213 Free PMC article.
-
Pathology in metopic synostosis.Childs Nerv Syst. 2013 Dec;29(12):2165-70. doi: 10.1007/s00381-013-2284-4. Epub 2013 Oct 3. Childs Nerv Syst. 2013. PMID: 24092422 Review.
-
Metopic synostosis.Childs Nerv Syst. 2012 Sep;28(9):1359-67. doi: 10.1007/s00381-012-1803-z. Epub 2012 Aug 8. Childs Nerv Syst. 2012. PMID: 22872249 Free PMC article. Review.
References
-
- Kweldam C F, van der Vlugt J J, van der Meulen J J. The incidence of craniosynostosis in the Netherlands, 1997-2007. J Plast Reconstr Aesthet Surg. 2011;64(5):583–588. - PubMed
-
- Anderson F M. Treatment of coronal and metopic synostosis: 107 cases. Neurosurgery. 1981;8(2):143–149. - PubMed
-
- Shillito J Jr, Matson D D. Craniosynostosis: a review of 519 surgical patients. Pediatrics. 1968;41(4):829–853. - PubMed
-
- Collmann H, Sörensen N, Krauss J. Consensus: trigonocephaly. Childs Nerv Syst. 1996;12(11):664–668. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
