

18F-Fluorodeoxyglucose positron emission tomography/CT scanning in diagnosing vascular prosthetic graft infection
- PMID: 25210712
- PMCID: PMC4156987
- DOI: 10.1155/2014/471971
18F-Fluorodeoxyglucose positron emission tomography/CT scanning in diagnosing vascular prosthetic graft infection
Abstract
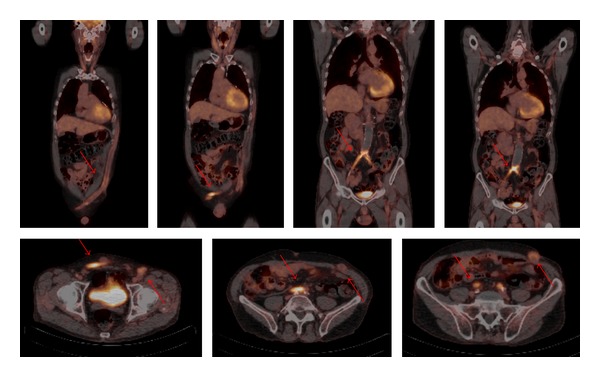
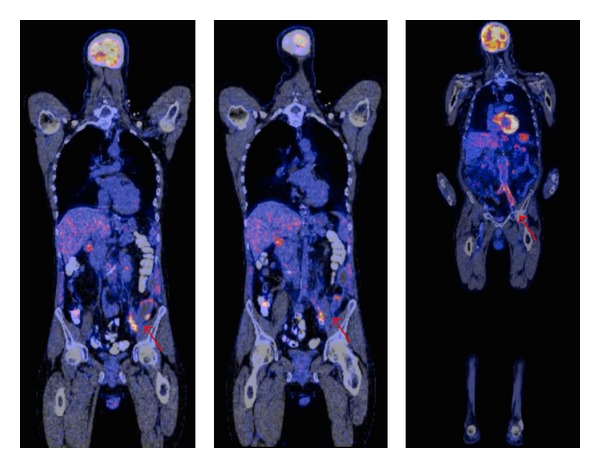
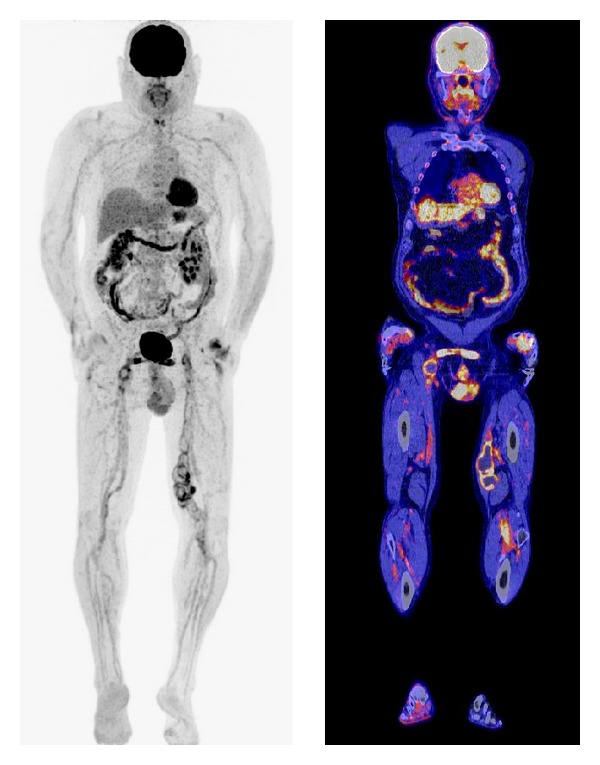
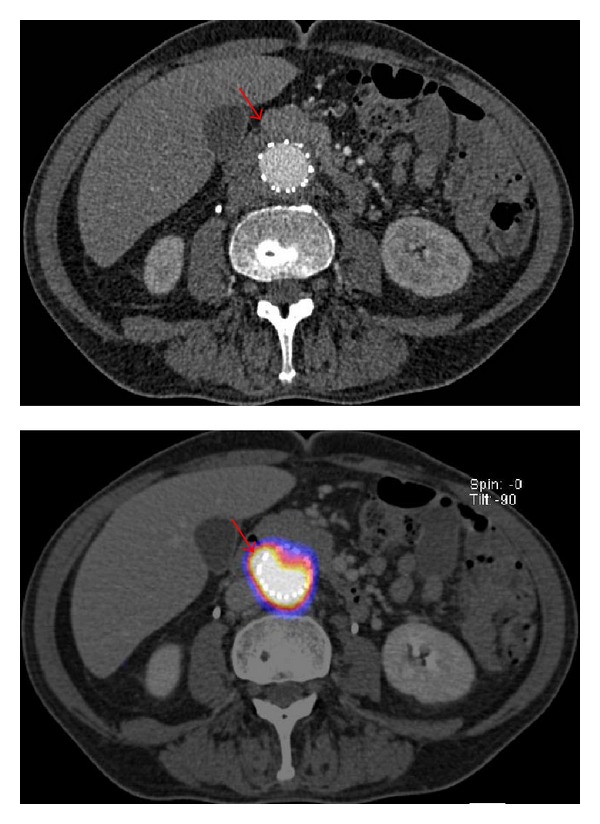
Vascular prosthetic graft infection (VPGI) is a severe complication after vascular surgery. CT-scan is considered the diagnostic tool of choice in advanced VPGI. The incidence of a false-negative result using CT is relatively high, especially in the presence of low-grade infections. (18)F-fluorodeoxyglucose positron emission tomography ((18)F-FDG PET) scanning has been suggested as an alternative for the diagnosis and assessment of infectious processes. Hybrid (18)F-FDG PET/CT has established the role of (18)F-FDG PET for the assessment of suspected VPGI, providing accurate anatomic localization of the site of infection. However, there are no clear guidelines for the interpretation of the uptake patterns of (18)F-FDG as clinical tool for VPGI. Based on the available literature it is suggested that a linear, diffuse, and homogeneous uptake should not be regarded as an infection whereas focal or heterogeneous uptake with a projection over the vessel on CT is highly suggestive of infection. Nevertheless, (18)F-FDG PET and (18)F-FDG PET/CT can play an important role in the detection of VPGI and monitoring response to treatment. However an accurate uptake and pattern recognition is warranted and cut-off uptake values and patterns need to be standardized before considering the technique to be the new standard.
Figures
References
-
- Saleem BR, Meerwaldt R, Tielliu IFJ, Verhoeven ELG, van den Dungen JJAM, Zeebregts CJ. Conservative treatment of vascular prosthetic graft infection is associated with high mortality. The American Journal of Surgery. 2010;200(1):47–52. - PubMed
-
- Legout L, D'Elia PV, Sarraz-Bournet B, et al. Diagnosis and management of prosthetic vascular graft infections. Medecine et Maladies Infectieuses. 2012;42(3):102–109. - PubMed
-
- Keidar Z, Nitecki S. FDG-PET in prosthetic graft infections. Seminars in Nuclear Medicine. 2013;43(5):396–402. - PubMed
-
- Swain TW, III, Calligaro KD, Dougherty MD. Management of infected aortic prosthetic grafts. Vascular and Endovascular Surgery. 2004;38(1):75–82. - PubMed
-
- Valentine RJ. Diagnosis and management of aortic graft infection. Seminars in Vascular Surgery. 2001;14(4):292–301. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
