

Impact of a community-based lymphedema management program on episodes of Adenolymphangitis (ADLA) and lymphedema progression--Odisha State, India
- PMID: 25211334
- PMCID: PMC4161333
- DOI: 10.1371/journal.pntd.0003140
Impact of a community-based lymphedema management program on episodes of Adenolymphangitis (ADLA) and lymphedema progression--Odisha State, India
Abstract
Background: Lymphedema management programs have been shown to decrease episodes of adenolymphangitis (ADLA), but the impact on lymphedema progression and of program compliance have not been thoroughly explored. Our objectives were to determine the rate of ADLA episodes and lymphedema progression over time for patients enrolled in a community-based lymphedema management program. We explored the association between program compliance and ADLA episodes as well as lymphedema progression.
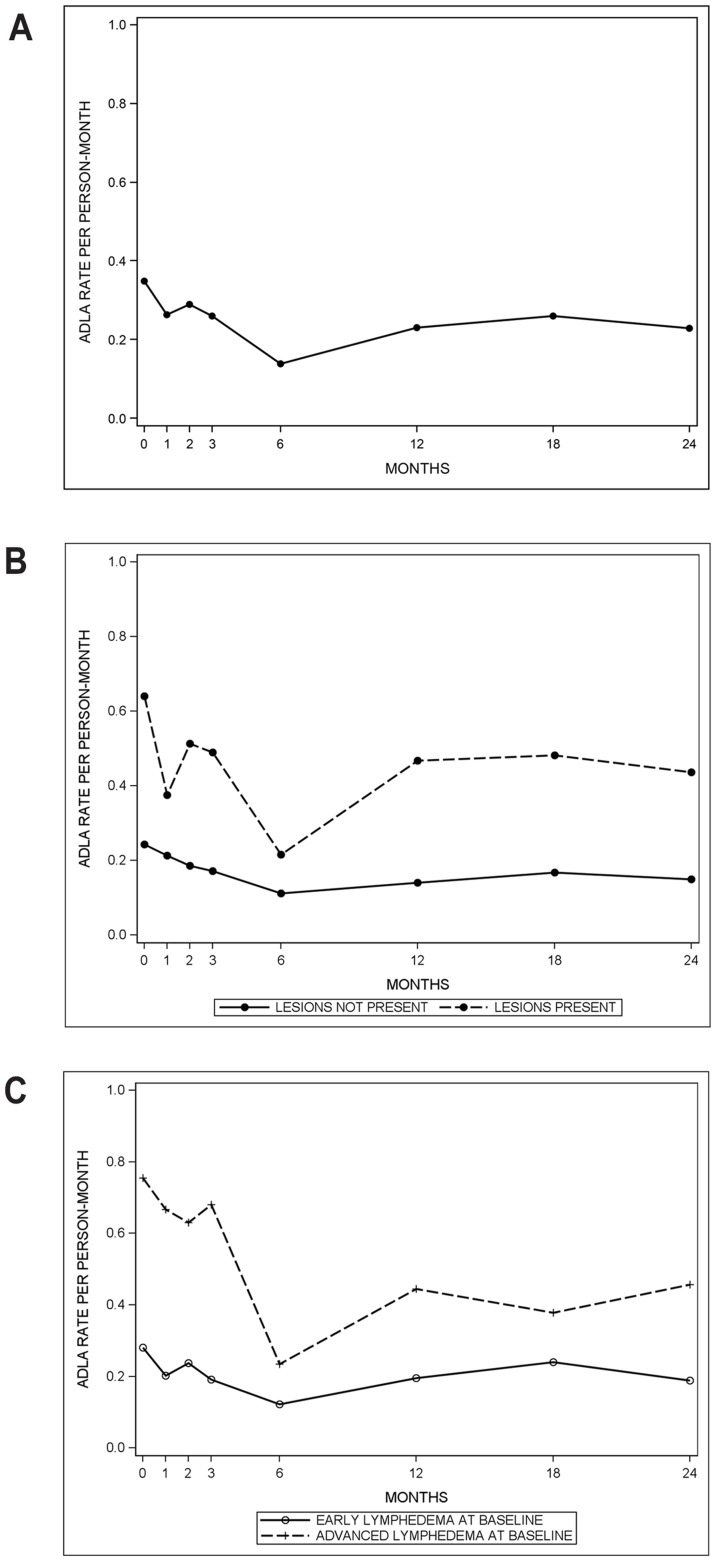
Methodology/principal findings: A lymphedema management program was implemented in Odisha State, India from 2007-2010 by the non-governmental organization, Church's Auxiliary for Social Action, in consultation with the Centers for Disease Control and Prevention. A cohort of patients was followed over 24 months. The crude 30-day rate of ADLA episodes decreased from 0.35 episodes per person-month at baseline to 0.23 at 24 months. Over the study period, the percentage of patients who progressed to more severe lymphedema decreased (P-value = 0.0004), while those whose lymphedema regressed increased over time (P-value<0.0001). Overall compliance to lymphedema management, lagged one time point, appeared to have little to no association with the frequency of ADLA episodes among those without entry lesions (RR = 0.87 (0.69, 1.10)) and was associated with an increased rate (RR = 1.44 (1.11, 1.86)) among those with entry lesions. Lagging compliance two time points, it was associated with a decrease in the rate of ADLA episodes among those with entry lesions (RR = 0.77 (95% CI: 0.59, 0.99)) and was somewhat associated among those without entry lesions (RR = 0.83 (95% CI: 0.64, 1.06)). Compliance to soap was associated with a decreased rate of ADLA episodes among those without inter-digital entry lesions.
Conclusions/significance: These results indicate that a community-based lymphedema management program is beneficial for lymphedema patients for both ADLA episodes and lymphedema. It is one of the first studies to demonstrate an association between program compliance and rate of ADLA episodes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Nutman TB, Kazura JW (2011) Lymphatic Filariasis. In: Guerrant RL, Walker DH, Weller PF, editors. Tropical Infectious Diseases: Principles, Pathogens, and Practice. 3rd ed. Edinburgh, London, New York, Oxford, Philadelphia, St. Louis, Sydney, Toronto: Saunders Elsevier. pp. 729–734.
-
- Shenoy RK, Kumaraswami V, Suma TK, Rajan K, Radhakuttyamma G (1999) A double-blind, placebo-controlled study of the efficacy of oral penicillin, diethylcarbamazine or local treatment of the affected limb in preventing acute adenolymphangitis in lymphoedema caused by brugian filariasis. Ann Trop Med Parasitol 93: 367–377. - PubMed
-
- Shenoy RK, Suma TK, Rajan K, Kumaraswami V (1998) Prevention of acute adenolymphangitis in brugian filariasis: comparison of the efficacy of ivermectin and diethylcarbamazine, each combined with local treatment of the affected limb. Ann Trop Med Parasitol 92: 587–594. - PubMed
-
- Pani SP, Srividya A (1995) Clinical manifestations of bancroftian filariasis with special reference to lymphoedema grading. Indian J Med Res 102: 114–118. - PubMed
-
- Addiss DG, Michel MC, Michelus A, Radday J, Billhimer W, et al. (2011) Evaluation of antibacterial soap in the management of lymphoedema in Leogane, Haiti. Trans R Soc Trop Med Hyg 105: 58–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
