

Integrating stages of change models to cast new vision on interventions to improve global retinoblastoma and childhood cancer outcomes
- PMID: 25213666
- PMCID: PMC4165911
- DOI: 10.1186/1471-2458-14-944
Integrating stages of change models to cast new vision on interventions to improve global retinoblastoma and childhood cancer outcomes
Abstract
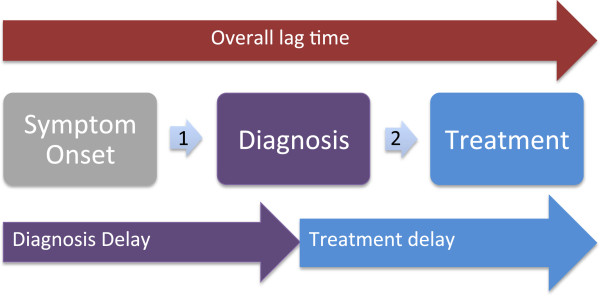
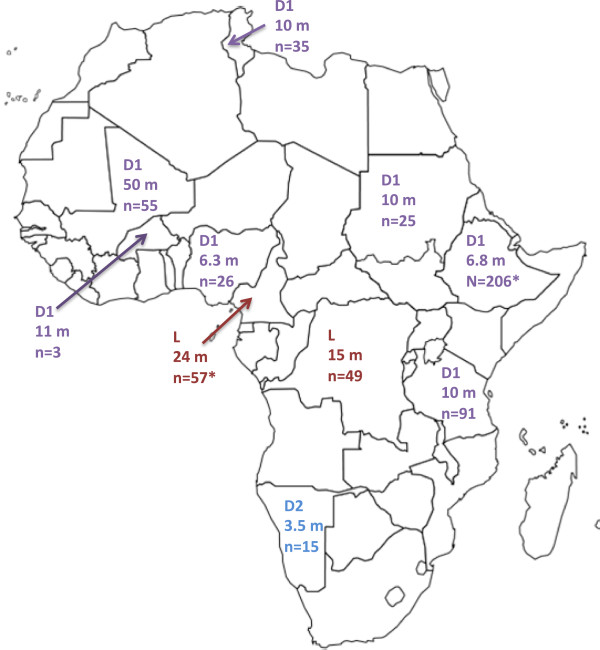
Background: Retinoblastoma, the most common intraocular tumor globally, represents a curable cancer when diagnosed early and treated promptly. Delay to diagnosis, lag time prior to treatment initiation, and abandonment of treatment including upfront treatment refusal, represent stark causes of high retinoblastoma mortality rates in low- and middle- income settings, particularly regions in Africa. While a health delivery-based approach has been a historic focus of retinoblastoma treatments globally and is essential to quality care, this is necessary but not adequate. Retinoblastoma is a compelling disease model to illustrate the potential insights afforded in theory-informed approaches to improve outcomes that integrate public health and oncology perspectives, prioritizing both health service delivery and social efficacy for cure.
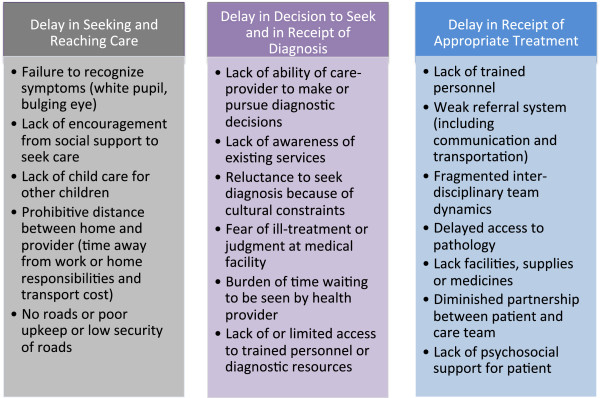
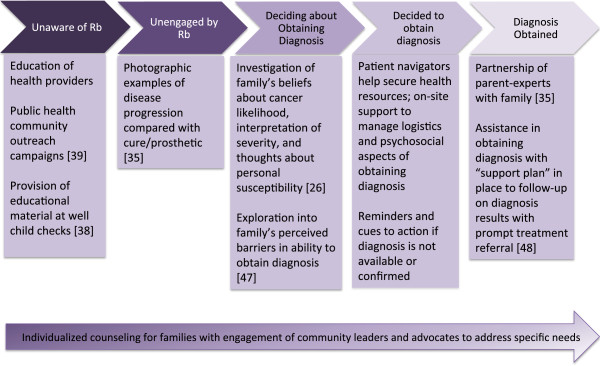
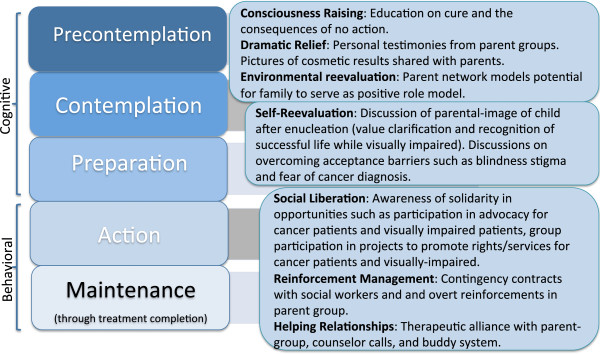
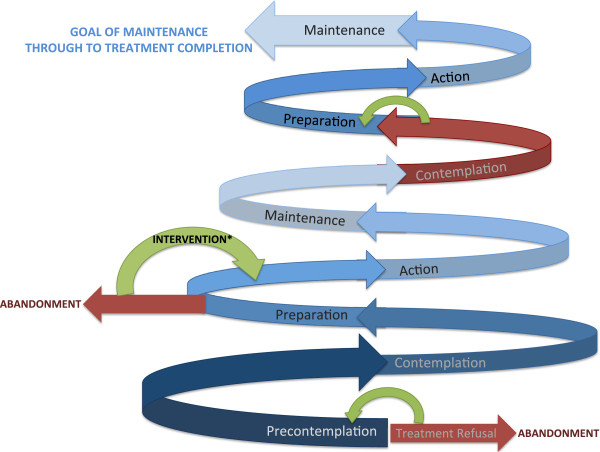
Discussion: Given that barriers to appropriate and timely diagnosis and treatment represent main contributors to mortality in children with retinoblastoma in resource-limited settings such as certain areas in Africa, an important priority is to overcome barriers to cure that may be predominantly socially influenced, alongside health delivery-based improvements. While Stages of Change models have been effectively utilized in cancer screening programs within settings of economic and cultural barriers, this application of health behavior theory has been limited to cancer screening rather than a comprehensive framework for treatment completion. Using retinoblastoma as a case example, we propose applying stage-based intervention models in critical stages of care, such as the Precaution Adoption Process Model to decrease delay to diagnosis and a Transtheoretical Model to increase treatment completion rates in resource-limited settings.
Summary: Stage-based theories recognize that improved cure and survival outcomes will require supportive strategies to progress households, communities, and social and economic institutions from being unaware and unengaged to committed and sustained in their respective roles. Applying a stage-based model lens to programmatic interventions in resource-limited settings has potential for visible improvement in outcomes for children with retinoblastoma and other cancers.
Figures
References
-
- Kivela T. The epidemiological challenge of the most frequent eye cancer: retinoblastoma, an issue of birth and death. Br J Ophthalmol. 2009;93(9):1129–1131. - PubMed
-
- Sachdeva S. Trend of reported cases of retinoblastoma under five hospital based cancer registries. Indian J Cancer. 2010;47(4):473–474. - PubMed
-
- Dimaras H, Kimani K, Dimba EA, Gronsdahl P, White A, Chan HS, Gallie BL. Retinoblastoma. Lancet. 2012;379(9824):1436–1446. - PubMed
-
- Rodriguez-Galindo C, Wilson MW, Chantada G, Fu L, Qaddoumi I, Antoneli C, Leal-Leal C, Sharma T, Barnoya M, Epelman S, Pizzarello L, Kane JR, Barfield R, Merchant TE, Robison LL, Murphree AL, Chevez-Barrios P, Dyer MA, O'Brien J, Ribeiro RC, Hungerford J, Helveston EM, Haik BG, Wilimas J. Retinoblastoma: one world, one vision. Pediatrics. 2008;122(3):e763–770. - PMC - PubMed
-
- Leal-Leal CA, Dilliz-Nava H, Flores-Rojo M, Robles-Castro J. First contact physicians and retinoblastoma in Mexico. Pediatr Blood Cancer. 2011;57(7):1109–1112. - PubMed
Pre-publication history
-
- The pre-publication history for this paper can be accessed here: http://www.biomedcentral.com/1471-2458/14/944/prepub
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
