

RV-pulmonary arterial coupling predicts outcome in patients referred for pulmonary hypertension
- PMID: 25214501
- PMCID: PMC4268056
- DOI: 10.1136/heartjnl-2014-306142
RV-pulmonary arterial coupling predicts outcome in patients referred for pulmonary hypertension
Abstract
Objective: Prognosis in pulmonary hypertension (PH) is largely determined by RV function. However, uncertainty remains about what metrics of RV function might be most clinically relevant. The purpose of this study was to assess the clinical relevance of metrics of RV functional adaptation to increased afterload.
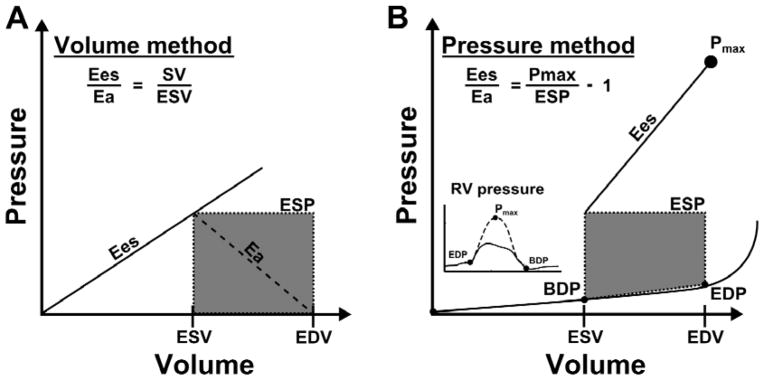
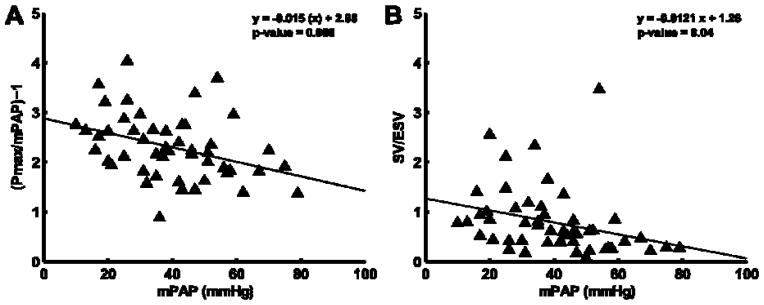
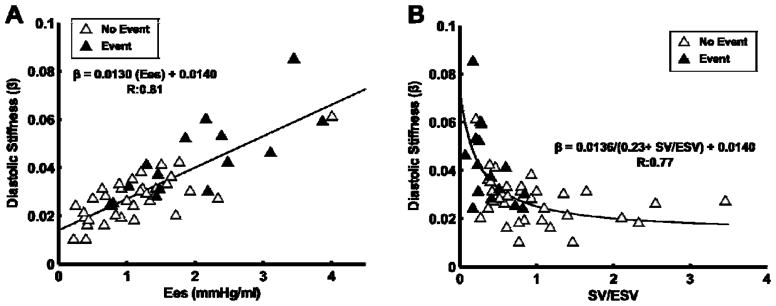
Methods: Patients referred for PH underwent right heart catheterisation and RV volumetric assessment within 48 h. A RV maximum pressure (Pmax) was calculated from the RV pressure curve. The adequacy of RV systolic functional adaptation to increased afterload was estimated either by a stroke volume (SV)/end-systolic volume (ESV) ratio, a Pmax/mean pulmonary artery pressure (mPAP) ratio, or by EF (RVEF). Diastolic function of the RV was estimated by a diastolic elastance coefficient β. Survival analysis was via Cox proportional HR, and Kaplan-Meier with the primary outcome of time to death or lung transplant.
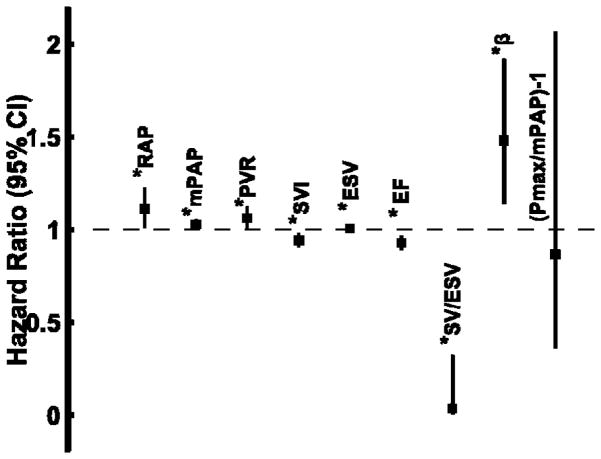
Results: Patients (n=50; age 58±13 yrs) covered a range of mPAP (13-79 mm Hg) with an average RVEF of 39±17% and ESV of 143±89 mL. Average estimates of the ratio of end-systolic ventricular to arterial elastance were 0.79±0.67 (SV/ESV) and 2.3±0.65 (Pmax/mPAP-1). Transplantation-free survival was predicted by right atrial pressure, mPAP, pulmonary vascular resistance, β, SV, ESV, SV/ESV and RVEF, but after controlling for right atrial pressure, mPAP, and SV, SV/ESV was the only independent predictor.
Conclusions: The adequacy of RV functional adaptation to afterload predicts survival in patients referred for PH. Whether this can simply be evaluated using RV volumetric imaging will require additional confirmation.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Dr. Simon reports receiving research funding from Pfizer. Dr. Vanderpool reports receiving consulting fees from United Therapeutics. Dr. Mathier reports receiving research funding from Actelion, consulting fees or serving on paid advisory boards for Gilead and Actelion and receiving lecture fees from Actelion, Encysive, and GlaxoSmithKline. Drs. Lacomis and Deible report receiving research funding from MEDRAD Inc. Dr. Champion reports receiving consulting fees or serving on paid advisory boards for Gilead, United Therapeutics, Bayer, Merck and Pfizer. Dr. Pinsky, Mr. Kosaraju, and Ms. Bunner have no competing interests.
Figures


References
-
- Sagawa K, Maughan L, Suga H, et al. Cardiac contraction and the pressure-volume relationship. New York: Oxford University Press; 1988.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical