

Effect of biofilms on recalcitrance of staphylococcal joint infection to antibiotic treatment
- PMID: 25214518
- PMCID: PMC4318921
- DOI: 10.1093/infdis/jiu514
Effect of biofilms on recalcitrance of staphylococcal joint infection to antibiotic treatment
Abstract
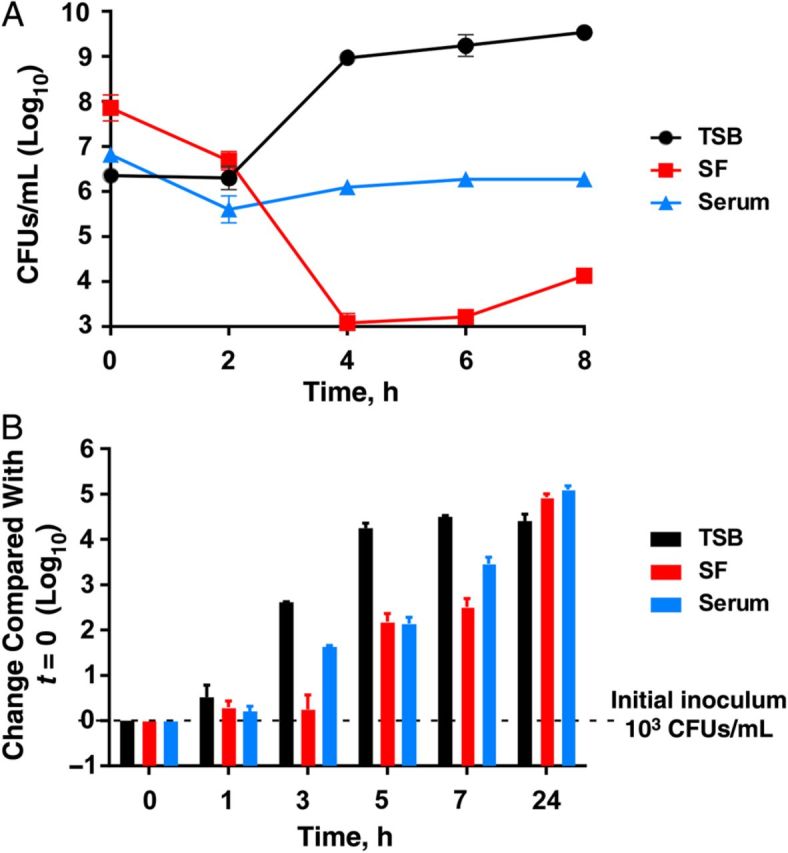
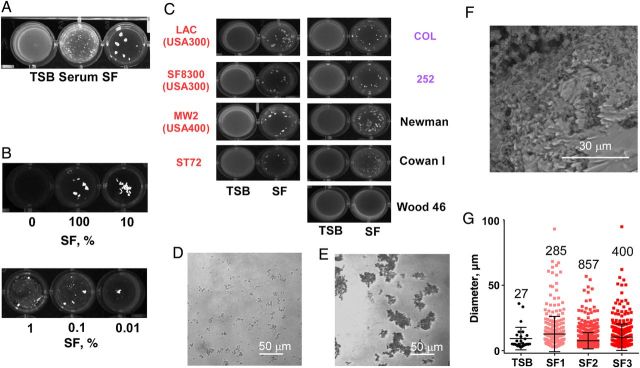
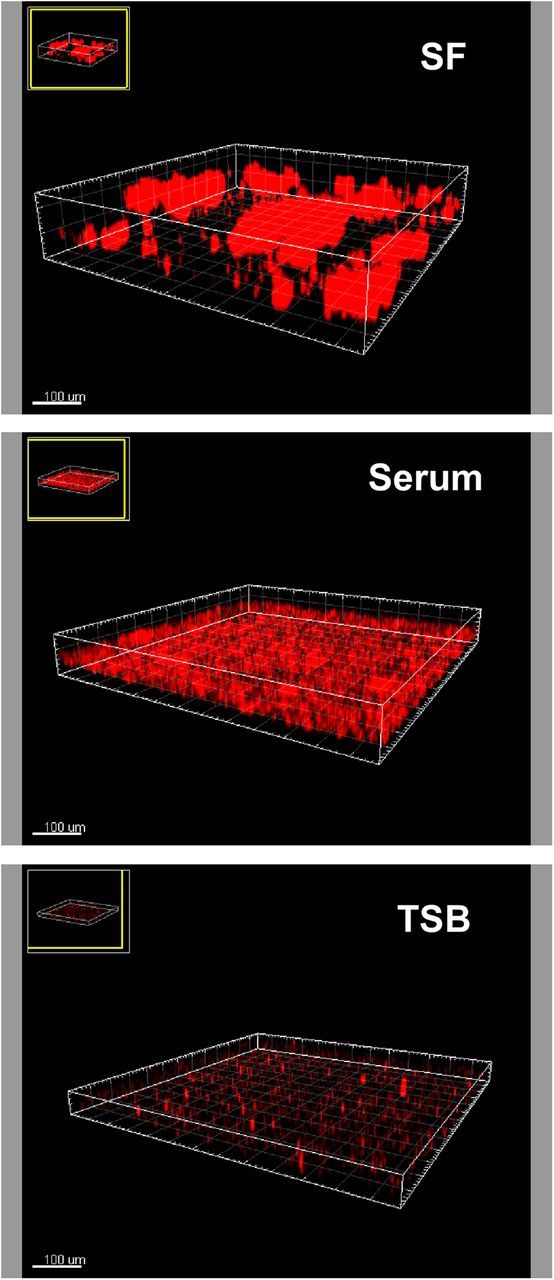
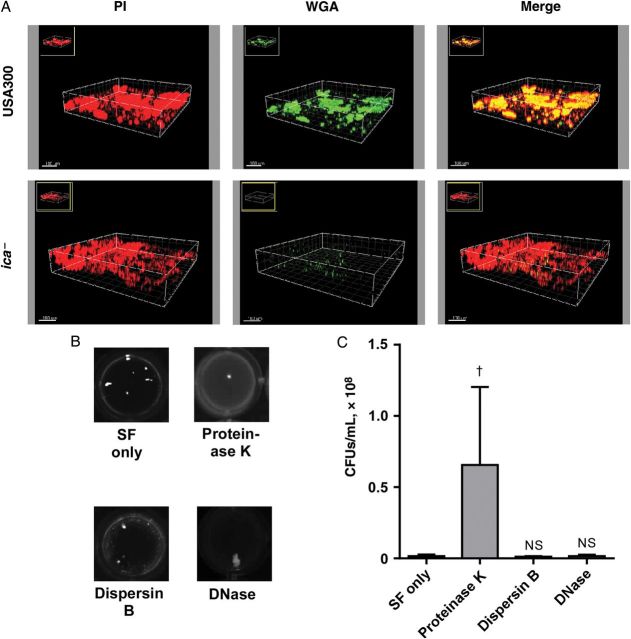
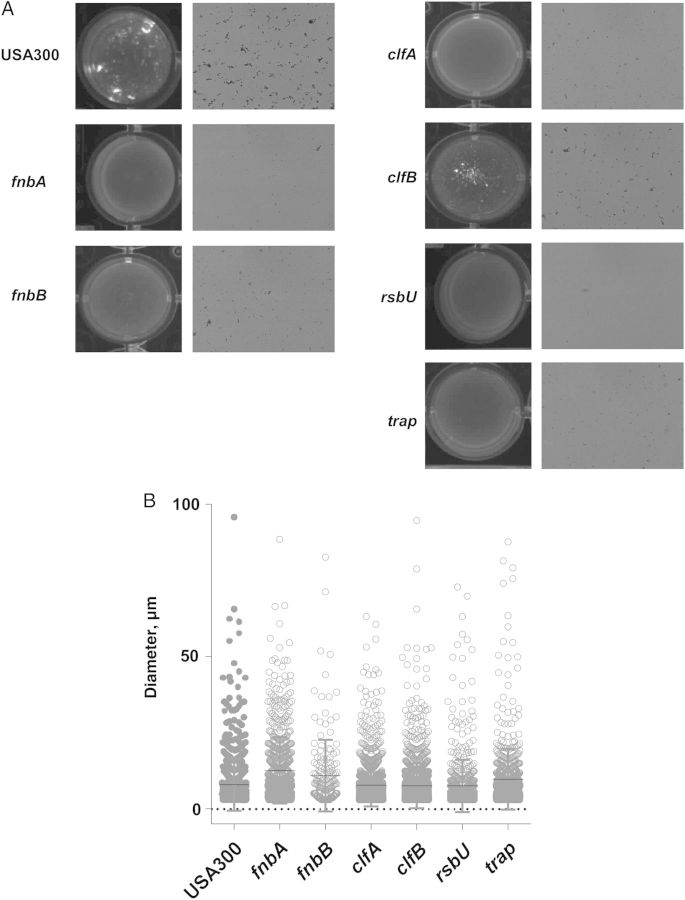
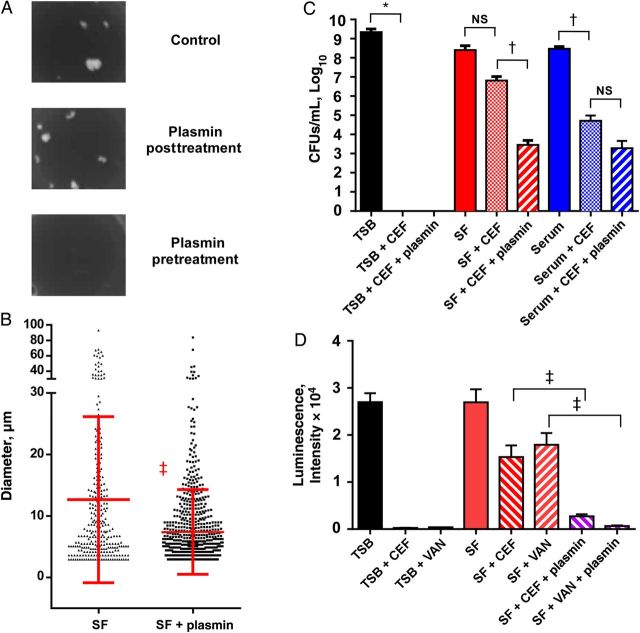
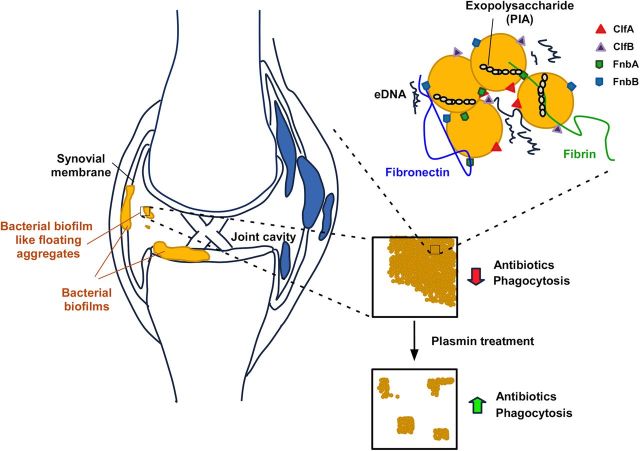
The pathogenesis of joint infections is not well understood. In particular, we do not know why these infections respond poorly to antibiotic treatment. Here we show that methicillin-resistant Staphylococcus aureus, a major cause of joint infections, forms exceptionally strong biofilmlike aggregates in human synovial fluid (SF), to an extent significantly exceeding biofilm formation observed in growth medium or serum. Screening a transposon bank identified bacterial fibronectin- and fibrinogen-binding proteins as important for the formation of macroscopic clumps in SF, suggesting an important role of fibrin-containing clots in the formation of bacterial aggregates during joint infection. Pretreatment of SF with plasmin led to a strongly reduced formation of aggregates and increased susceptibility to antibiotics. These results give important insight into the pathogenesis of staphylococcal joint infection and the mechanisms underlying resistance to treatment. Furthermore, they point toward a potential novel approach for treating joint infections.
Keywords: MRSA; Staphylococcus aureus; antibiotic resistance; biofilm; joint infection; septic arthritis.
Published by Oxford University Press on behalf of the Infectious Diseases Society of America 2014. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures
Comment in
-
Biofilm-like aggregation of Staphylococcus epidermidis in synovial fluid.J Infect Dis. 2015 Jul 15;212(2):335-6. doi: 10.1093/infdis/jiv096. Epub 2015 Feb 23. J Infect Dis. 2015. PMID: 25712965 Free PMC article. No abstract available.
-
Reply to Perez and Patel.J Infect Dis. 2015 Jul 15;212(2):336-7. doi: 10.1093/infdis/jiv097. Epub 2015 Feb 23. J Infect Dis. 2015. PMID: 25712972 Free PMC article. No abstract available.
References
-
- Zimmerli W, Trampuz A, Ochsner PE. Prosthetic-joint infections. N Engl J Med. 2004;351:1645–54. - PubMed
-
- Lora-Tamayo J, Murillo O, Iribarren JA, et al. A large multicenter study of methicillin-susceptible and methicillin-resistant Staphylococcus aureus prosthetic joint infections managed with implant retention. Clin Infect Dis. 2013;56:182–94. - PubMed
-
- Salgado CD, Dash S, Cantey JR, Marculescu CE. Higher risk of failure of methicillin-resistant Staphylococcus aureus prosthetic joint infections. Clin Orthop Relat Res. 2007;461:48–53. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
