

Evaluating the management of anaphylaxis in US emergency departments: Guidelines vs. practice
- PMID: 25215101
- PMCID: PMC4129832
- DOI: 10.5847/wjem.j.issn.1920-8642.2013.02.003
Evaluating the management of anaphylaxis in US emergency departments: Guidelines vs. practice
Abstract
Background: Anaphylaxis is characterized by acute episodes of potentially life-threatening symptoms that are often treated in the emergency setting. Current guidelines recommend: 1) quick diagnosis using standard criteria; 2) first-line treatment with epinephrine; and 3) discharge with a prescription for an epinephrine auto-injector, written instructions regarding long-term management, and a referral (preferably, allergy) for follow-up. However, studies suggest low concordance with guideline recommendations by emergency medicine (EM) providers. The study aimed to evaluate how emergency departments (EDs) in the United States (US) manage anaphylaxis in relation to guideline recommendations.
Methods: This was an online anonymous survey of a random sample of EM health providers in US EDs.
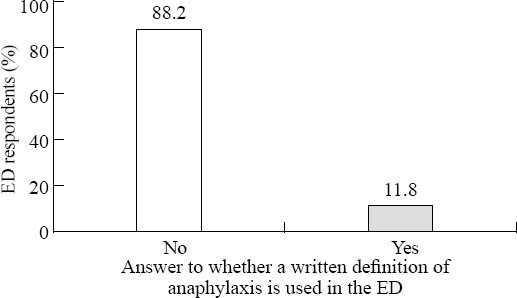
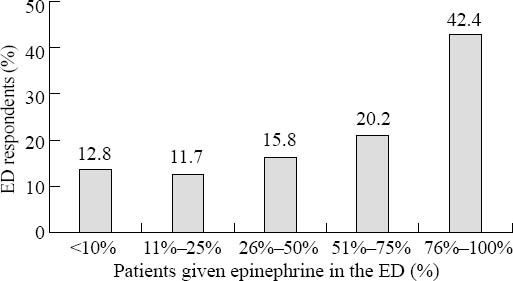
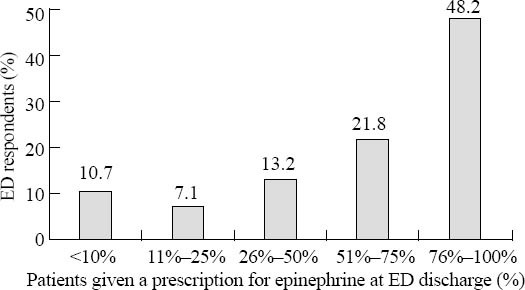
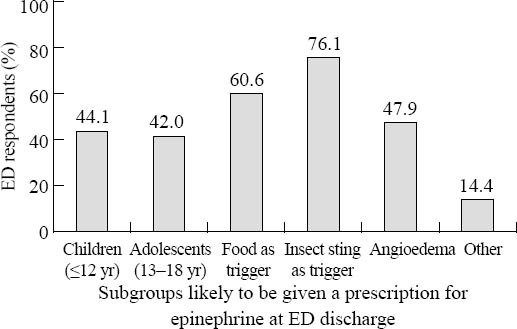
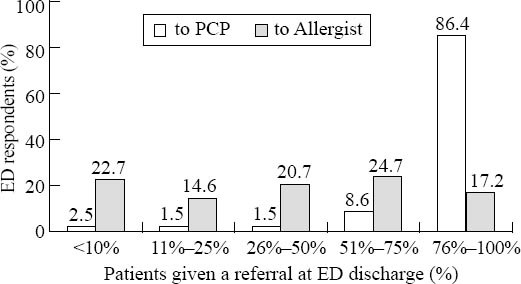
Results: Data analysis included 207 EM providers. For respondent EDs, approximately 9% reported using agreed-upon clinical criteria to diagnose anaphylaxis; 42% reported administering epinephrine in the ED for most anaphylaxis episodes; and <50% provided patients with a prescription for an epinephrine auto-injector and/or an allergist referral on discharge. Most provided some written materials, and follow-up with a primary care clinician was recommended.
Conclusions: This is the first cross-sectional survey to provide "real-world" data showing that practice in US EDs is discordant with current guideline recommendations for the diagnosis, treatment, and follow-up of patients with anaphylaxis. The primary gaps are low (or no) utilization of standard criteria for defining anaphylaxis and inconsistent use of epinephrine. Prospective research is recommended.
Keywords: Allergic reaction; Anaphylaxis; Emergency department; Epinephrine (adrenaline); Epinephrine autoinjector; Guidelines; Life-threatening reaction; Self-injectable epinephrine.
Conflict of interest statement
Figures
Similar articles
-
Changes in Emergency Department Concordance with Guidelines for the Management of Food-Induced Anaphylaxis: 1999-2001 versus 2013-2015.J Allergy Clin Immunol Pract. 2019 Sep-Oct;7(7):2262-2269. doi: 10.1016/j.jaip.2019.04.004. Epub 2019 Apr 8. J Allergy Clin Immunol Pract. 2019. PMID: 30974210
-
Changes in emergency department concordance with guidelines for the management of stinging insect-induced anaphylaxis: 1999-2001 vs 2013-2015.Ann Allergy Asthma Immunol. 2018 Apr;120(4):419-423. doi: 10.1016/j.anai.2018.01.029. Ann Allergy Asthma Immunol. 2018. PMID: 29407420
-
Anaphylaxis management in a French pediatric emergency department: Lessons from the ANA-PED study.Clin Transl Allergy. 2023 Aug;13(8):e12289. doi: 10.1002/clt2.12289. Clin Transl Allergy. 2023. PMID: 37632240 Free PMC article.
-
[The use of adrenaline for the treatment of anaphylaxis: the use by first-aid personnel is recommended].Presse Med. 2013 Jun;42(6 Pt 1):922-9. doi: 10.1016/j.lpm.2012.11.012. Epub 2013 Mar 6. Presse Med. 2013. PMID: 23474047 Review. French.
-
Review article: quality of follow-up care for anaphylaxis in the emergency department.Emerg Med Australas. 2015 Oct;27(5):387-93. doi: 10.1111/1742-6723.12458. Epub 2015 Aug 28. Emerg Med Australas. 2015. PMID: 26315372 Review.
Cited by
-
Under Prescription of Epinephrine to Medicaid Patients in the Pediatric Emergency Department.Glob Pediatr Health. 2019 Jun 13;6:2333794X19854960. doi: 10.1177/2333794X19854960. eCollection 2019. Glob Pediatr Health. 2019. PMID: 31236431 Free PMC article.
-
Anaphylaxis in America: A national physician survey.J Allergy Clin Immunol. 2015 Mar;135(3):830-3. doi: 10.1016/j.jaci.2014.10.049. Epub 2015 Jan 7. J Allergy Clin Immunol. 2015. PMID: 25577592 Free PMC article. No abstract available.
-
How to define severity: A review of allergic reaction severity scoring systems.Ann Allergy Asthma Immunol. 2023 Aug;131(2):170-175. doi: 10.1016/j.anai.2023.05.009. Epub 2023 May 19. Ann Allergy Asthma Immunol. 2023. PMID: 37209834 Free PMC article. Review.
-
Triage Grading and Correct Diagnosis Are Critical for the Emergency Treatment of Anaphylaxis.Children (Basel). 2022 Nov 23;9(12):1794. doi: 10.3390/children9121794. Children (Basel). 2022. PMID: 36553239 Free PMC article.
-
Minimizing the "Kitchen Sink" Approach: De-implementation of Unnecessary Care for Patients with Anaphylaxis in a Pediatric Emergency Department.Pediatr Qual Saf. 2022 Mar 30;7(2):e535. doi: 10.1097/pq9.0000000000000535. eCollection 2022 Mar-Apr. Pediatr Qual Saf. 2022. PMID: 35369411 Free PMC article.
References
-
- Bohlke K, Davis RI, DeStefano F, Marcy SM, Braun MM, Thompson RS, et al. Epidemiology of anaphylaxis among children and adolescents enrolled in a health maintenance organization. J Allergy Clin Immunol. 2004;113:536–542. - PubMed
-
- Clark S, Camargo CA., Jr Epidemiology of anaphylaxis. Immunol Allergy Clin N Am. 2007;27:145–163. - PubMed
-
- Lieberman P, Nicklas RA, Oppenheimer J, Kemp SF, Lang DM, Bernstein DI, et al. The diagnosis and management of anaphylaxis practice parameter: 2010 update. J Allergy Clin Immunol. 2010;126:477–480. - PubMed
-
- Sampson HA, Munoz-Furlong A, Campbell R, Adkinson NF, Jr, Bock SA, Branum A, et al. Second symposium on the definition and management of anaphylaxis: summary report. Ann Emerg Med. 2006;47:373–380. Also published in J Allergy Clin Immunol 2006; 117: 391-397. - PubMed
LinkOut - more resources
Full Text Sources