

doi: 10.1155/2014/273423.
Epub 2014 Aug 19.
Pheochromocytoma in a Twelve-Year-Old Girl with SDHB-Related Hereditary Paraganglioma-Pheochromocytoma Syndrome
Affiliations
- PMID: 25215250
- PMCID: PMC4156988
- DOI: 10.1155/2014/273423
Item in Clipboard
Pheochromocytoma in a Twelve-Year-Old Girl with SDHB-Related Hereditary Paraganglioma-Pheochromocytoma Syndrome
Case Rep Genet.
2014.
Abstract
A twelve-year-old girl presented with a history of several weeks of worsening headaches accompanied by flushing and diaphoresis. The discovery of markedly elevated blood pressure and tachycardia led the child's pediatrician to consider the diagnosis of a catecholamine-secreting tumor, and an abdominal CT scan confirmed the presence of a pheochromocytoma. The patient was found to have a mutation in the succinyl dehydrogenase B (SDHB) gene, which is causative for SDHB-related hereditary paraganglioma-pheochromocytoma syndrome. Herein, we describe her presentation and medical management and discuss the clinical implications of SDHB deficiency.
Figures
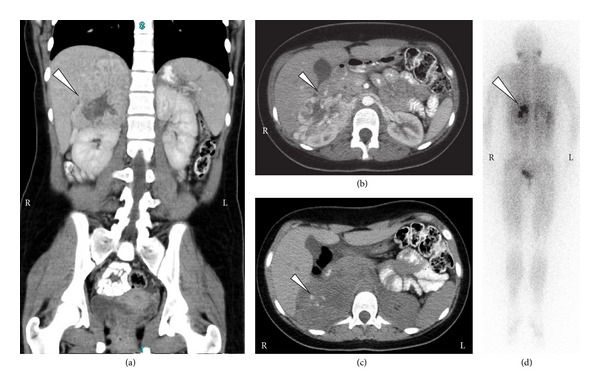
Radiologic imaging of the patient at presentation. (a, b, c) Computed tomography images showing a right-sided contrast-enhancing suprarenal mass (white arrows) displacing both the kidney and the liver. Note calcifications in the mass (arrow; image (c)), which is typical for pheochromocytoma. (d) MIBG nuclear scan showing uptake by the adrenal mass (arrow) and no evidence of other sites of disease.
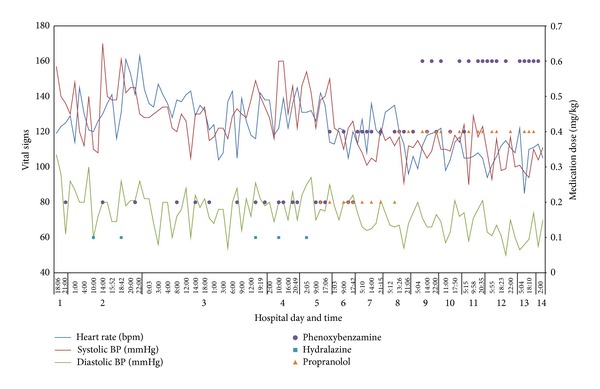
Sympathetic blockade and vital signs. Clinical data showing heart rate, systolic blood pressure, and diastolic blood pressure from admission until the time of tumor resection. Also shown are anticatecholamine medications and their doses over time. Note the progressive decreases in hypertension and tachycardia over the patient's hospital course.
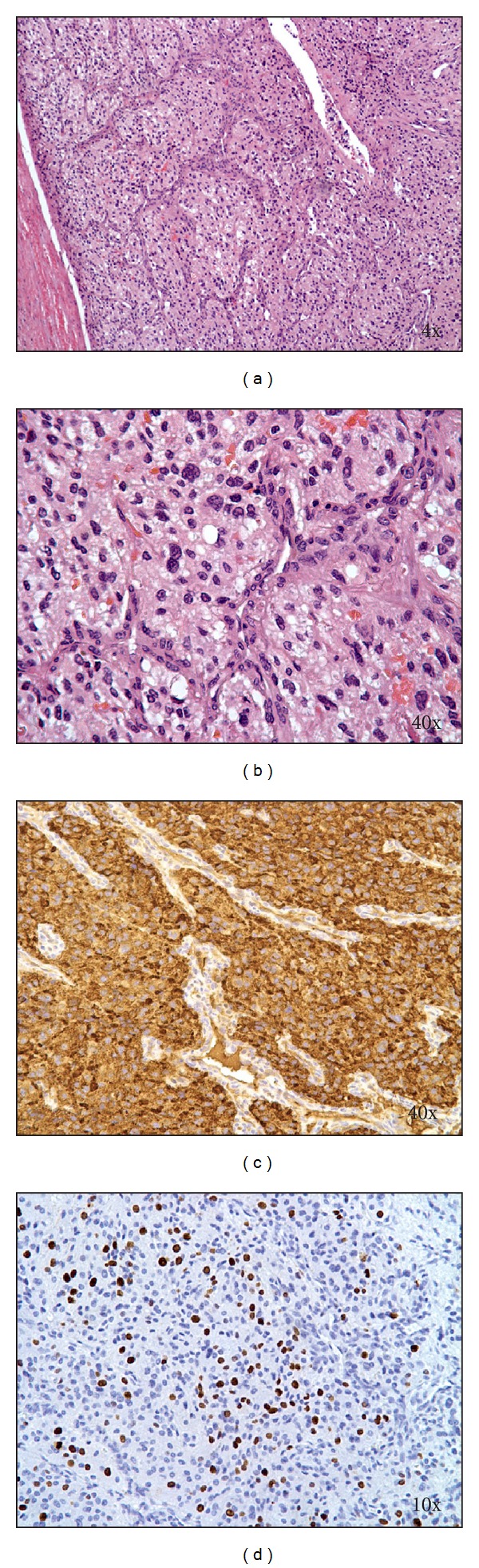
Pathologic images of resected tumor. (a, b) H & E-stained sections of the tumor showing tumor cells with abundant eosinophilic cytoplasm arranged in a nested and trabecular pattern and surrounded by fibrovascular stroma. (c) Chromogranin A staining demonstrating strong positivity of tumor cells. (d) Ki67 (MIB-1) immunostaining confirmed a high proliferation index (>10%) of the tumor cell population.
Similar articles
-
A Novel SDHB IVS2-2A>C Mutation Is Responsible for Hereditary Pheochromocytoma/Paraganglioma Syndrome.Tohoku J Exp Med. 2018 Jun;245(2):99-105. doi: 10.1620/tjem.245.99. Tohoku J Exp Med. 2018. PMID: 29925701
-
Loss of SDHB Elevates Catecholamine Synthesis and Secretion Depending on ROS Production and HIF Stabilization.Neurochem Res. 2016 Apr;41(4):696-706. doi: 10.1007/s11064-015-1738-3. Epub 2015 Nov 30. Neurochem Res. 2016. PMID: 26620190
-
Mutation analysis of SDHB and SDHC: novel germline mutations in sporadic head and neck paraganglioma and familial paraganglioma and/or pheochromocytoma.BMC Med Genet. 2006 Jan 11;7:1. doi: 10.1186/1471-2350-7-1. BMC Med Genet. 2006. PMID: 16405730 Free PMC article.
-
Paraganglioma of the Vagina Associated With Germline SDHB Mutation: Report of a Case With Review of the Literature.Int J Gynecol Pathol. 2020 Nov;39(6):599-604. doi: 10.1097/PGP.0000000000000658. Int J Gynecol Pathol. 2020. PMID: 31851064 Review.
-
Temozolomide Is a Potential Therapeutic Tool for Patients With Metastatic Pheochromocytoma/Paraganglioma-Case Report and Review of the Literature.Front Endocrinol (Lausanne). 2020 Feb 18;11:61. doi: 10.3389/fendo.2020.00061. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 32132978 Free PMC article. Review.
Cited by
-
Mutation profiling in eight cases of vagal paragangliomas.BMC Med Genomics. 2020 Sep 18;13(Suppl 8):115. doi: 10.1186/s12920-020-00763-4. BMC Med Genomics. 2020. PMID: 32948195 Free PMC article.
-
Clinical Practice Guidance: Surveillance for phaeochromocytoma and paraganglioma in paediatric succinate dehydrogenase gene mutation carriers.Clin Endocrinol (Oxf). 2019 Apr;90(4):499-505. doi: 10.1111/cen.13926. Epub 2019 Jan 29. Clin Endocrinol (Oxf). 2019. PMID: 30589099 Free PMC article. Review.
References
-
- Neumann HP, Bausch B, McWhinney SR. Germ-line mutations in nonsyndromic pheochromocytoma. The New England Journal of Medicine. 2002;346(19):1459–1466. - PubMed
-
- Neumann HP, Pawlu C, Peczkowska M, et al. Distinct clinical features of paraganglioma syndromes associated with SDHB and SDHD gene mutations. The Journal of the American Medical Association. 2004;292(8):943–951. - PubMed
-
- McDonnell CM, Benn DE, Marsh DJ, Robinson BG, Zacharin MR. K40E: a novel succinate dehydrogenase (SDH)B mutation causing familial phaeochromocytoma and paraganglioma. Clinical Endocrinology. 2004;61(4):510–514. - PubMed
-
- Cascón A, Landa Í, López-Jiménez E, et al. Molecular characterisation of a common SDHB deletion in paraganglioma patients. Journal of Medical Genetics. 2008;45(4):233–238. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
