

Hepatosplenic sarcoidosis: contrast-enhanced ultrasound findings and implications for clinical practice
- PMID: 25215299
- PMCID: PMC4151864
- DOI: 10.1155/2014/926203
Hepatosplenic sarcoidosis: contrast-enhanced ultrasound findings and implications for clinical practice
Abstract
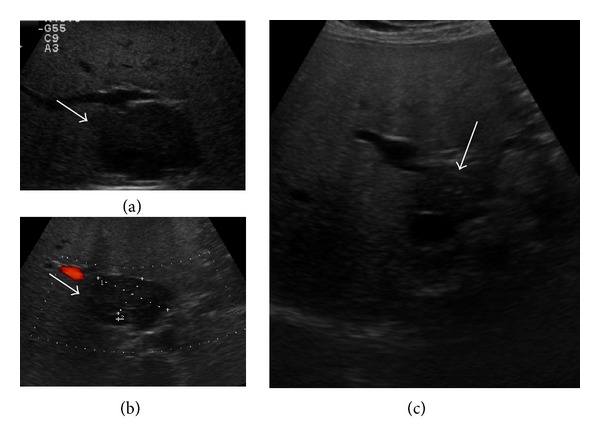
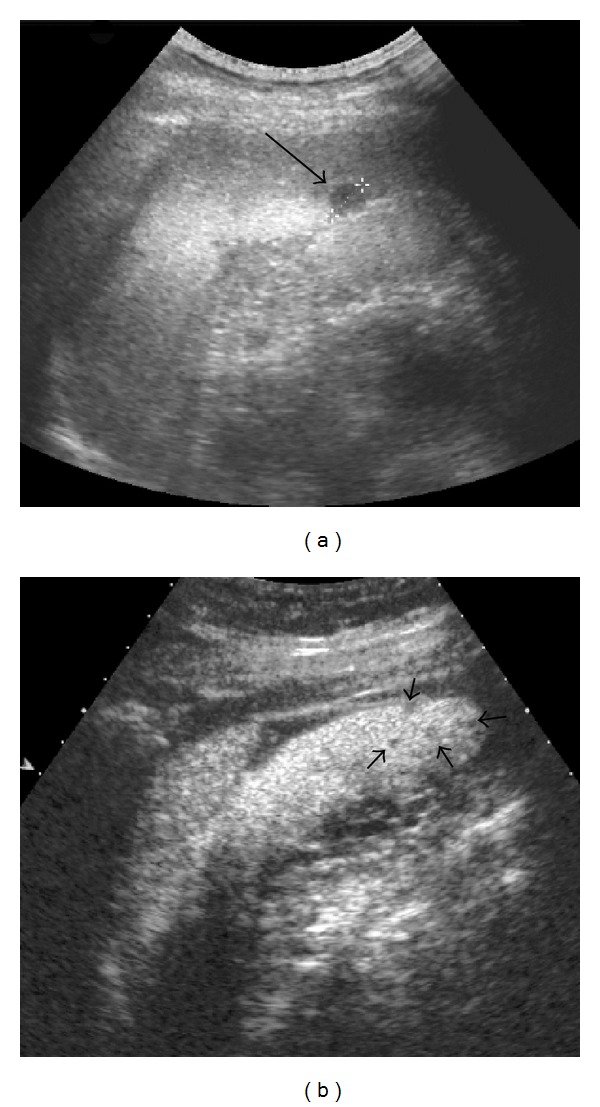
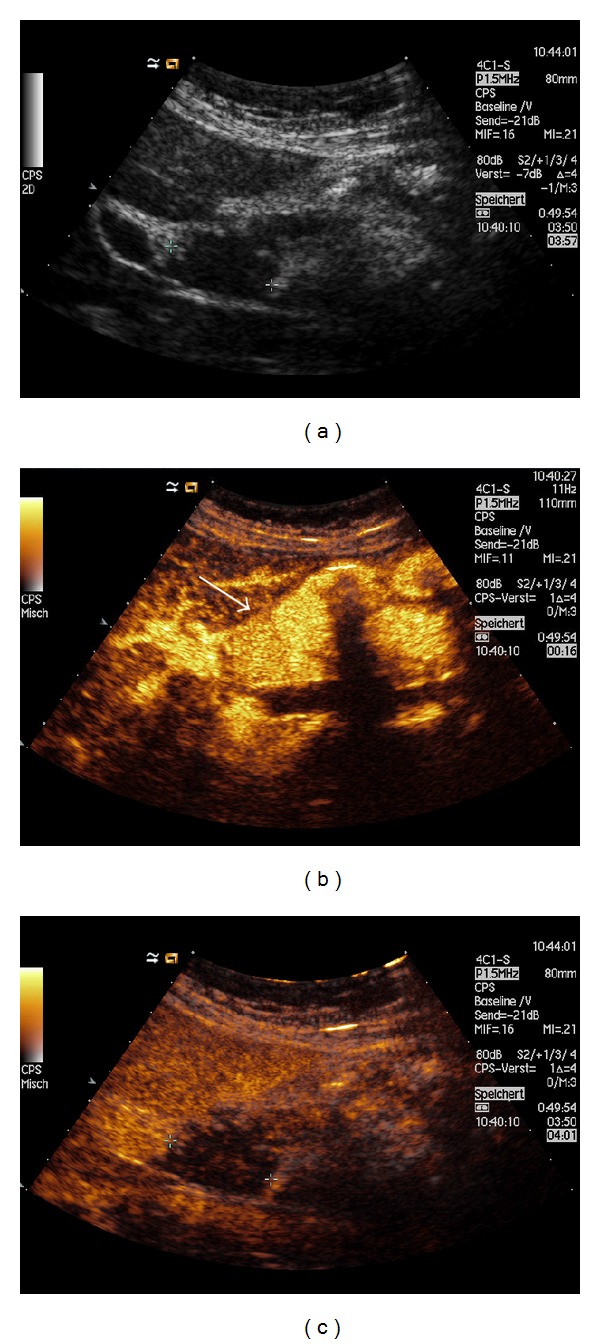
Sarcoidosis is a complex granulomatous disease that affects virtually every organ and tissue, with a prevalence that varies significantly among the sites involved. The role of conventional imaging, such as computed tomography and magnetic resonance imaging, in the assessment of hepatosplenic sarcoidosis is well established by revealing organ enlargement, multiple discrete nodules, and lymphadenopathy. In this review, we aim to describe contrast-enhanced ultrasound (CEUS) findings in liver and spleen involvement by sarcoidosis, reporting evidence from the literature and cases from our experience, after a brief update on safety profile, cost-effectiveness, and clinical indications of this novel technique. Furthermore, we highlight potential advantages of CEUS in assessing hepatosplenic sarcoidosis that may be useful in the clinical practice.
Figures


Similar articles
-
[Isolated sarcoidosis of the spleen and liver as incidental ultrasound finding].Rofo. 2010 Apr;182(4):353-4. doi: 10.1055/s-0028-1109829. Epub 2009 Oct 27. Rofo. 2010. PMID: 19862662 German. No abstract available.
-
Diagnostic potential of contrast-enhanced ultrasound (CEUS) in the assessment of spleen and liver granulomas in the course of sarcoidosis.Pneumonol Alergol Pol. 2013;81(5):424-8. Pneumonol Alergol Pol. 2013. PMID: 23996881
-
Contrast-enhanced ultrasonography in hepatosplenic sarcoidosis.Acta Clin Belg. 2011 Nov-Dec;66(6):429-31. doi: 10.2143/ACB.66.6.2062609. Acta Clin Belg. 2011. PMID: 22338306
-
CT patterns of nodular hepatic and splenic sarcoidosis: a review of the literature.J Comput Assist Tomogr. 1997 May-Jun;21(3):369-72. doi: 10.1097/00004728-199705000-00006. J Comput Assist Tomogr. 1997. PMID: 9135642 Review.
-
Hepatosplenic and muscular sarcoidosis: characterization with MR imaging.Magn Reson Med Sci. 2012;11(2):83-9. doi: 10.2463/mrms.11.83. Magn Reson Med Sci. 2012. PMID: 22790294 Review.
Cited by
-
Incidental Focal Spleen Lesions: Integrated Imaging and Pattern Recognition Approach to the Differential Diagnosis.Diagnostics (Basel). 2023 Jul 30;13(15):2536. doi: 10.3390/diagnostics13152536. Diagnostics (Basel). 2023. PMID: 37568899 Free PMC article. Review.
-
Insights Into Hepatic Sarcoidosis: Analysis of Histological Patterns, Hepatic Complications and Therapeutic Approaches.Liver Int. 2025 Mar;45(3):e70037. doi: 10.1111/liv.70037. Liver Int. 2025. PMID: 39969799 Free PMC article.
-
Two Cases with Isolated Splenic Sarcoidosis Diagnosed by an Ultrasound-guided Fine-needle Aspiration Biopsy.Intern Med. 2023 Jul 15;62(14):2077-2083. doi: 10.2169/internalmedicine.0409-22. Epub 2022 Nov 30. Intern Med. 2023. PMID: 36450462 Free PMC article.
-
[Hepatic granuloma-A diagnostic challenge].Z Rheumatol. 2022 Sep;81(7):567-576. doi: 10.1007/s00393-022-01235-z. Epub 2022 Jun 28. Z Rheumatol. 2022. PMID: 35763059 Review. German.
-
The Role of Echocardiography in the Contemporary Diagnosis and Prognosis of Cardiac Sarcoidosis: A Comprehensive Review.Life (Basel). 2023 Jul 29;13(8):1653. doi: 10.3390/life13081653. Life (Basel). 2023. PMID: 37629510 Free PMC article. Review.
References
-
- Iannuzzi MC, Rybicki BA, Teirstein AS. Sarcoidosis. The New England Journal of Medicine. 2007;357(21):2153–2165. - PubMed
-
- Iannuzzi MC, Fontana JR. Sarcoidosis: clinical presentation, immunopathogenesis, and therapeutics. Journal of the American Medical Association. 2011;305(4):391–399. - PubMed
-
- Valeyre D, Prasse A, Nunes H, Uzunhan Y, Brillet PY, Müller-Quernheim J. Sarcoidosis. The Lancet. 2014;383(9923):1155–1167. - PubMed
-
- Hirche TO, Hirche H, Cui XW, Wagner TO, Dietrich CF. Ultrasound evaluation of mediastinal lymphadenopathy in patients with sarcoidosis. Medical Ultrasonography. 2014;16(3):194–200. - PubMed
-
- Tana C, Giamberardino MA, Di Gioacchino M, Mezzetti A, Schiavone C. Immunopathogenesis of sarcoidosis and risk of malignancy: a lost truth? International Journal of Immunopathology and Pharmacology. 2013;26(2):305–313. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
