

Proceedings of the first international summit on intestinal anastomotic leak, Chicago, Illinois, October 4-5, 2012
- PMID: 25215465
- PMCID: PMC4382716
- DOI: 10.1089/sur.2013.114
Proceedings of the first international summit on intestinal anastomotic leak, Chicago, Illinois, October 4-5, 2012
Abstract
Objective: The first international summit on anastomotic leak was held in Chicago in October, 2012 to assess current knowledge in the field and develop novel lines of inquiry. The following report is a summary of the proceedings with commentaries and future prospects for clinical trials and laboratory investigations.
Background: Anastomotic leakage remains a devastating problem for the patient, and a continuing challenge to the surgeon operating on high-risk areas of the gastrointestinal tract such as the esophagus and rectum. Despite the traditional wisdom that anastomotic leak is because of technique, evidence to support this is weak-to-non-existent. Outcome data continue to demonstrate that expert high-volume surgeons working in high-volume centers continue to experience anastomotic leaks and that surgeons cannot predict reliably which patients will leak.
Methods: A one and one-half day summit was held and a small working group assembled to review current practices, opinions, scientific evidence, and potential paths forward to understand and decrease the incidence of anastomotic leak.
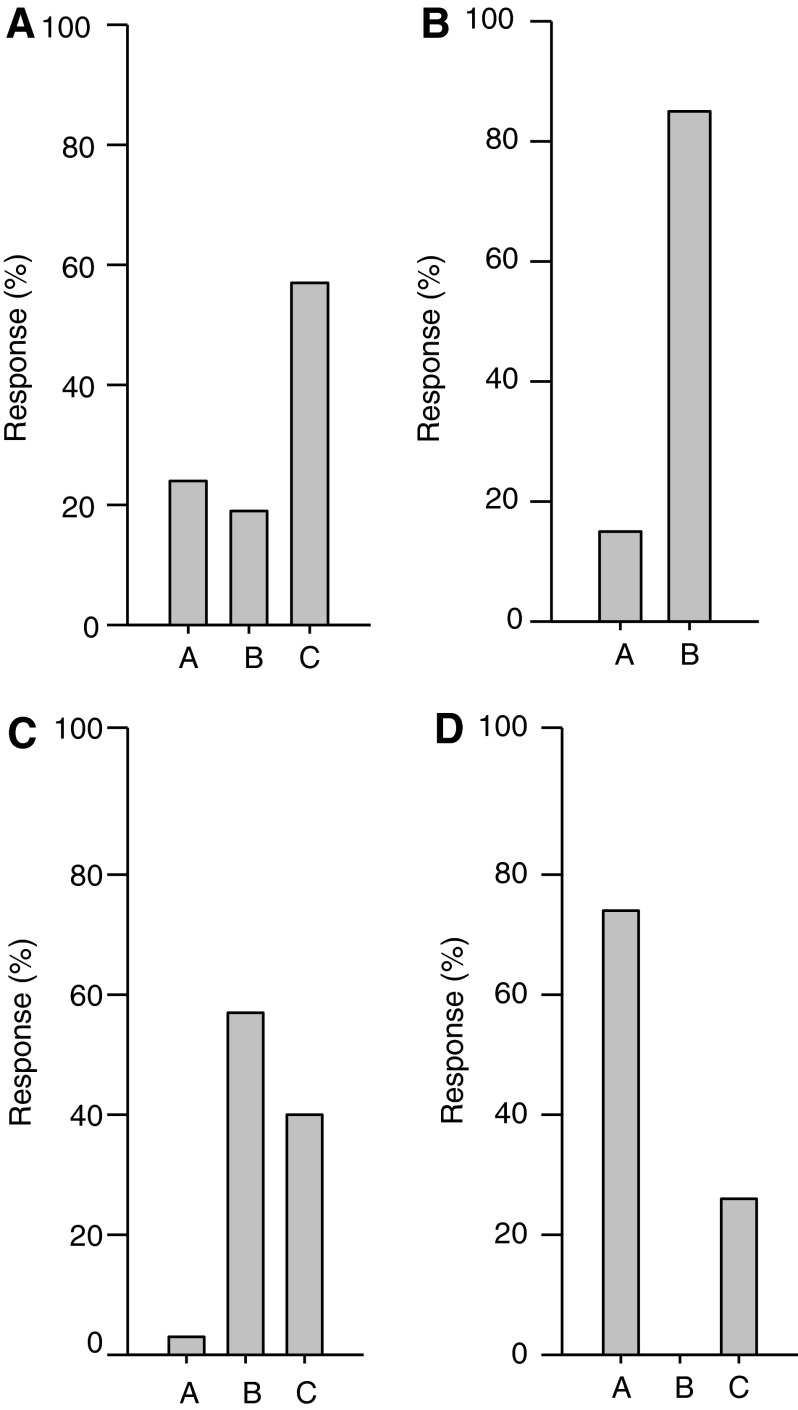
Results: RESULTS of a survey of the opinions of the group demonstrated that the majority of participants believe that anastomotic leak is a complicated biologic problem whose pathogenesis remains ill-defined. The group opined that anastomotic leak is underreported clinically, it is not because of technique except when there is gross inattention to it, and that results from animal models are mostly irrelevant to the human condition.
Conclusions: A fresh and unbiased examination of the causes and strategies for prevention of anastomotic leak needs to be addressed by a continuous working group of surgeons, basic scientists, and clinical trialists to realize a real and significant reduction in its incidence and morbidity. Such a path forward is discussed.
Figures
References
-
- Slim K, Panis Y, Chipponi J. Half of the currecnt practice of gastrointestinal surgery is against the evidence: A survey of the French Society of Digestive Surgery. J Gastrointest Surg 2004;8:1079–1082 - PubMed
-
- Ioannidis JP. Contradicted and initially stronger effects in highly cited clinical research. JAMA 2005;294:218–228 - PubMed
-
- Bruce J, Krukowski ZH, Al-Khairy G, et al. Systematic review of the definition and measurement of anastomotic leak after gastrointestinal surgery. Brit Journal Surg 2001;88:1157–1168 - PubMed
-
- Wright CD, Kucharczuk JC, O'Brien SM, et al. Predictors of major morbidity and mortality after esophagectomy for esophageal cancer: a Society of Thoracic Surgeons General Thoracic Surgery Database risk adjustment model. J Thorac Cardiovasc Surg 2009;137:587–595 - PubMed
-
- Kube R, Mroczkowski P, Steinert R, et al. [Anastomotic leakage following bowel resections for colon cancer: Multivariate analysis of risk factors]. Chirurg 2009;80:1153–1159 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
