

Clinical applications of wavefront refraction
- PMID: 25216319
- PMCID: PMC4186736
- DOI: 10.1097/OPX.0000000000000377
Clinical applications of wavefront refraction
Abstract
Purpose: To determine normative reference ranges for higher-order wavefront error (HO-WFE), compare these values with those in common ocular pathologies, and evaluate treatments.
Methods: A review of 17 major studies on HO-WFE was made, involving data for a total of 31,605 subjects. The upper limit of the 95% confidence interval (CI) for HO-WFE was calculated from the most comprehensive of these studies using normal healthy patients aged 20 to 80 years. There were no studies identified using the natural pupil size for subjects, and for this reason, the HO-WFE was tabulated for pupil diameters of 3 to 7 mm. Effects of keratoconus, pterygium, cataract, and dry eye on HO-WFE were reviewed and treatment efficacy was considered.
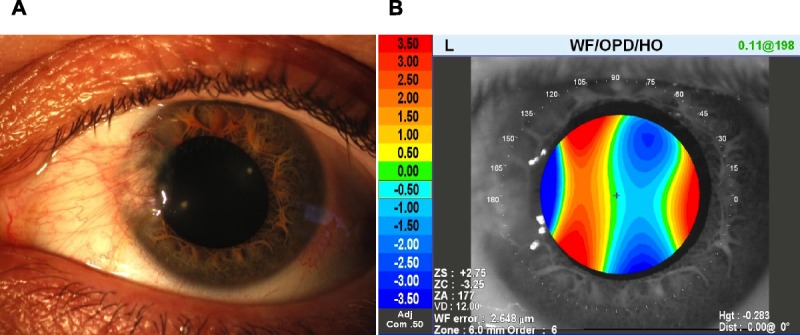
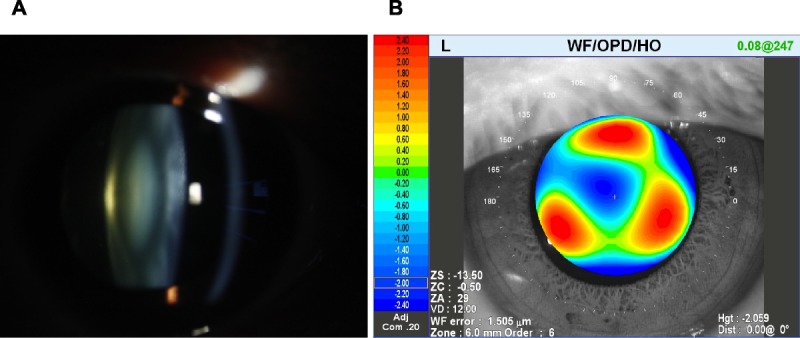
Results: The calculated upper limit of the 95% CI for HO-WFE in a healthy normal 35-year-old patient with a mesopic pupil diameter of 6 mm would be 0.471 μm (471 nm) root-mean-square or less. Although the normal HO-WFE increases with age for a given pupil size, it is not yet completely clear how the concurrent influence of age-related pupillary miosis affects these findings. Abnormal ocular conditions such as keratoconus can induce a large HO-WFE, often in excess of 3.0 μm, particularly attributed to coma. For pterygium or cortical cataract, a combination of coma and trefoil was more commonly induced. Nuclear cataract can induce a negative spherical HO-WFE, usually in excess of 1.0 μm.
Conclusions: The upper limit of the 95% CI for HO-WFE root-mean-square is about 0.5 μm with normal physiological pupil sizes. With ocular pathologies, HO-WFE can be in excess of 1.0 μm, although many devices and therapeutic and surgical treatments are reported to be highly effective at minimizing HO-WFE. More accurate normative reference ranges for HO-WFE will require future studies using the subjects' natural pupil size.
Figures


Similar articles
-
Three-dimensional relationship between high-order root-mean-square wavefront error, pupil diameter, and aging.J Opt Soc Am A Opt Image Sci Vis. 2007 Mar;24(3):578-87. doi: 10.1364/josaa.24.000578. J Opt Soc Am A Opt Image Sci Vis. 2007. PMID: 17301847 Free PMC article.
-
Noise in wavefront error measurement from pupil center location uncertainty.J Refract Surg. 2010 Oct;26(10):796-802. doi: 10.3928/1081597X-20100921-05. J Refract Surg. 2010. PMID: 20954688 Free PMC article.
-
Effects of a semi-scleral contact lens on refraction and higher order aberrations.Cont Lens Anterior Eye. 2019 Dec;42(6):670-674. doi: 10.1016/j.clae.2019.06.002. Epub 2019 Jun 21. Cont Lens Anterior Eye. 2019. PMID: 31230973
-
Detecting significant change in wavefront error: how long does it take?Clin Exp Optom. 2009 May;92(3):246-52. doi: 10.1111/j.1444-0938.2009.00368.x. Clin Exp Optom. 2009. PMID: 19469015 Free PMC article.
-
Alignment of a wavefront-guided scleral lens correction in the presence of a lens capsulotomy.Cont Lens Anterior Eye. 2020 Dec;43(6):613-616. doi: 10.1016/j.clae.2020.02.006. Epub 2020 Mar 4. Cont Lens Anterior Eye. 2020. PMID: 32146116 Free PMC article.
Cited by
-
Response to: Clinical results of topography-guided laser-assisted in situ keratomileusis using the anterior corneal astigmatism axis and manifest refractive astigmatism axis.Graefes Arch Clin Exp Ophthalmol. 2023 Mar;261(3):893-896. doi: 10.1007/s00417-022-05860-x. Epub 2022 Oct 20. Graefes Arch Clin Exp Ophthalmol. 2023. PMID: 36264334 No abstract available.
-
Assessment of refractive astigmatism and simulated therapeutic refractive surgery strategies in coma-like-aberrations-dominant corneal optics.Eye Vis (Lond). 2016 May 12;3:13. doi: 10.1186/s40662-016-0044-8. eCollection 2016. Eye Vis (Lond). 2016. PMID: 27175371 Free PMC article.
-
Evaluation of the Performance of Algorithm-Based Methods for Subjective Refraction.J Clin Med. 2020 Sep 29;9(10):3144. doi: 10.3390/jcm9103144. J Clin Med. 2020. PMID: 33003297 Free PMC article.
-
Ultra-High Resolution Optical Aberrometry in Patients with Keratoconus: A Cross-Sectional Study.Ophthalmol Ther. 2023 Jun;12(3):1569-1582. doi: 10.1007/s40123-023-00684-2. Epub 2023 Mar 1. Ophthalmol Ther. 2023. PMID: 36856979 Free PMC article.
-
Large dynamic range autorefraction with a low-cost diffuser wavefront sensor.Biomed Opt Express. 2019 Mar 7;10(4):1718-1735. doi: 10.1364/BOE.10.001718. eCollection 2019 Apr 1. Biomed Opt Express. 2019. PMID: 31061764 Free PMC article.
References
-
- Thibos LN, Himebaugh NL, Coe CD. Wavefront refraction. In: Benjamin WJ, Borish IM, eds. Borish’s Clinical Refraction, 2nd ed. Oxford, UK: Butterworth-Heinemann; 2006: 765– 89
-
- Krueger RR, Rabinowitz YS, Binder PS. The 25th anniversary of excimer lasers in refractive surgery: historical review. J Refract Surg 2010; 26: 749– 60 - PubMed
-
- Thibos LN. The 2012 Charles Prentice medal lecture: wavefront measurement of refractive state. Optom Vis Sci 2013; 90: 911– 23 - PubMed
-
- Thibos LN, Hong X, Bradley A, Cheng X. Statistical variation of aberration structure and image quality in a normal population of healthy eyes. J Opt Soc Am (A) 2002; 19: 2329– 48 - PubMed
-
- Rocha KM, Nosé W, Bottós K, Bottós J, Morimoto L, Soriano E. Higher-order aberrations of age-related cataract. J Cataract Refract Surg 2007; 33: 1442– 6 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
