

The tell-tale heart: molecular and cellular responses to childhood anthracycline exposure
- PMID: 25217655
- PMCID: PMC4233297
- DOI: 10.1152/ajpheart.00099.2014
The tell-tale heart: molecular and cellular responses to childhood anthracycline exposure
Abstract
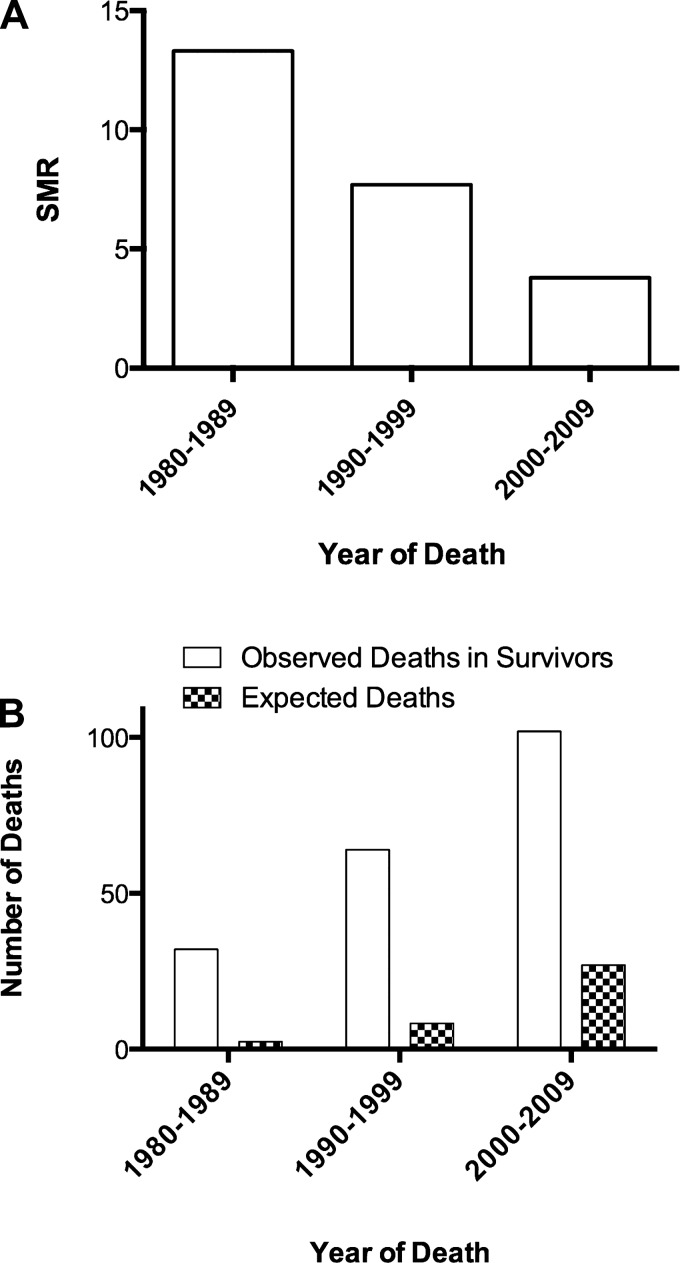
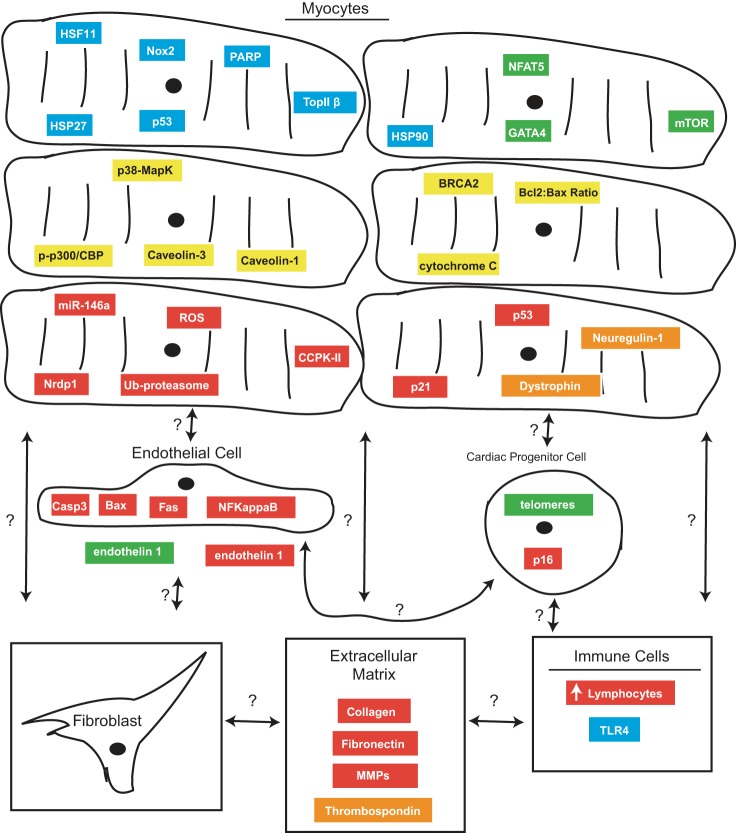
Since the modern era of cancer chemotherapy that began in the mid-1940s, survival rates for children afflicted with cancer have steadily improved from 10% to current rates that approach 80% (60). Unfortunately, many long-term survivors of pediatric cancer develop chemotherapy-related health effects; 25% are afflicted with a severe or life-threatening medical condition, with cardiovascular disease being a primary risk (96). Childhood cancer survivors have markedly elevated incidences of stroke, congestive heart failure (CHF), coronary artery disease, and valvular disease (96). Their cardiac mortality is 8.2 times higher than expected (93). Anthracyclines are a key component of most curative chemotherapeutic regimens used in pediatric cancer, and approximately half of all childhood cancer patients are exposed to them (78). Numerous epidemiologic and observational studies have linked childhood anthracycline exposure to an increased risk of developing cardiomyopathy and CHF, often decades after treatment. The acute toxic effects of anthracyclines on cardiomyocytes are well described; however, myocardial tissue is comprised of additional resident cell types, and events occurring in the cardiomyocyte do not fully explain the pathological processes leading to late cardiomyopathy and CHF. This review will summarize the current literature regarding the cellular and molecular responses to anthracyclines, with an important emphasis on nonmyocyte cardiac cell types as well as those that mediate the myocardial injury response.
Keywords: anthracyclines; cardiomyocytes; cardiomyopathy; congestive heart failure; extracellular matrix; fibroblast.
Copyright © 2014 the American Physiological Society.
Figures
Similar articles
-
New signal transduction paradigms in anthracycline-induced cardiotoxicity.Biochim Biophys Acta. 2016 Jul;1863(7 Pt B):1916-25. doi: 10.1016/j.bbamcr.2016.01.021. Epub 2016 Jan 29. Biochim Biophys Acta. 2016. PMID: 26828775 Review.
-
Mechanisms of anthracycline cardiac injury: can we identify strategies for cardioprotection?Prog Cardiovasc Dis. 2010 Sep-Oct;53(2):105-13. doi: 10.1016/j.pcad.2010.06.007. Prog Cardiovasc Dis. 2010. PMID: 20728697 Free PMC article. Review.
-
Anthracycline cardiotoxicity in long-term survivors of childhood cancer.Cardiovasc Toxicol. 2007;7(2):122-8. doi: 10.1007/s12012-007-0006-4. Cardiovasc Toxicol. 2007. PMID: 17652816 Review.
-
Cardiotoxicity of Cancer Treatments: Focus on Anthracycline Cardiomyopathy.Arterioscler Thromb Vasc Biol. 2021 Nov;41(11):2648-2660. doi: 10.1161/ATVBAHA.121.316697. Epub 2021 Sep 30. Arterioscler Thromb Vasc Biol. 2021. PMID: 34587760 Free PMC article. Review.
-
Anthracycline Chemotherapy and Cardiotoxicity.Cardiovasc Drugs Ther. 2017 Feb;31(1):63-75. doi: 10.1007/s10557-016-6711-0. Cardiovasc Drugs Ther. 2017. PMID: 28185035 Free PMC article. Review.
Cited by
-
Fibroblasts: The arbiters of extracellular matrix remodeling.Matrix Biol. 2020 Sep;91-92:1-7. doi: 10.1016/j.matbio.2020.05.006. Epub 2020 Jun 3. Matrix Biol. 2020. PMID: 32504772 Free PMC article. Review.
-
Doxorubicin-induced p53 interferes with mitophagy in cardiac fibroblasts.PLoS One. 2020 Sep 22;15(9):e0238856. doi: 10.1371/journal.pone.0238856. eCollection 2020. PLoS One. 2020. PMID: 32960902 Free PMC article.
-
Doxorubicin-Induced Cardiomyopathy in Children.Compr Physiol. 2019 Jun 12;9(3):905-931. doi: 10.1002/cphy.c180017. Compr Physiol. 2019. PMID: 31187890 Free PMC article. Review.
-
Left Ventricular Aneurysm Presenting as a Late Complication of Childhood Chemotherapy.Case Rep Cardiol. 2015;2015:625451. doi: 10.1155/2015/625451. Epub 2015 Sep 10. Case Rep Cardiol. 2015. PMID: 26448882 Free PMC article.
-
Factors associated with long-term cardiac dysfunction in neonatal lupus.Ann Rheum Dis. 2020 Feb;79(2):217-224. doi: 10.1136/annrheumdis-2019-215900. Epub 2019 Oct 31. Ann Rheum Dis. 2020. PMID: 31672776 Free PMC article.
References
-
- Al-Abd AM, Al-Abbasi FA, Asaad GF, Abdel-Naim AB. Didox potentiates the cytotoxic profile of doxorubicin and protects from its cardiotoxicity. Eur J Pharmacol 718: 361–369, 2013. - PubMed
-
- Alkreathy HM, Damanhouri ZA, Ahmed N, Slevin M, Osman AM. Mechanisms of cardioprotective effect of aged garlic extract against Doxorubicin-induced cardiotoxicity. Integr Cancer Ther 11: 364–370, 2012. - PubMed
-
- Ammar el-SM, Said SA, Suddek GM, El-Damarawy SL. Amelioration of doxorubicin-induced cardiotoxicity by deferiprone in rats. Can J Physiol Pharmacol 89: 269–276, 2011. - PubMed
-
- Ammar HI, Saba S, Ammar RI, Elsayed LA, Ghaly WB, Dhingra S. Erythropoietin protects against doxorubicin-induced heart failure. Am J Physiol Heart Circ Physiol 301: H2413–H2421, 2011. - PubMed
-
- Arbel Y, Swartzon M, Justo D. QT prolongation and Torsades de Pointes in patients previously treated with anthracyclines. Anticancer Drugs 18: 493–498, 2007. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical