

An activating NLRC4 inflammasome mutation causes autoinflammation with recurrent macrophage activation syndrome
- PMID: 25217959
- PMCID: PMC4177369
- DOI: 10.1038/ng.3089
An activating NLRC4 inflammasome mutation causes autoinflammation with recurrent macrophage activation syndrome
Abstract
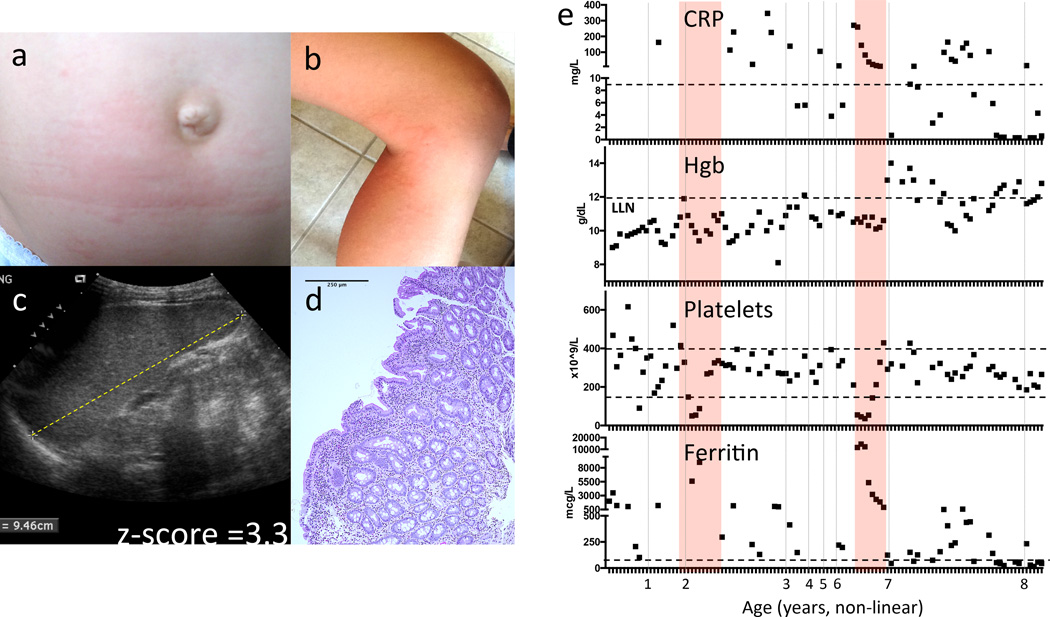
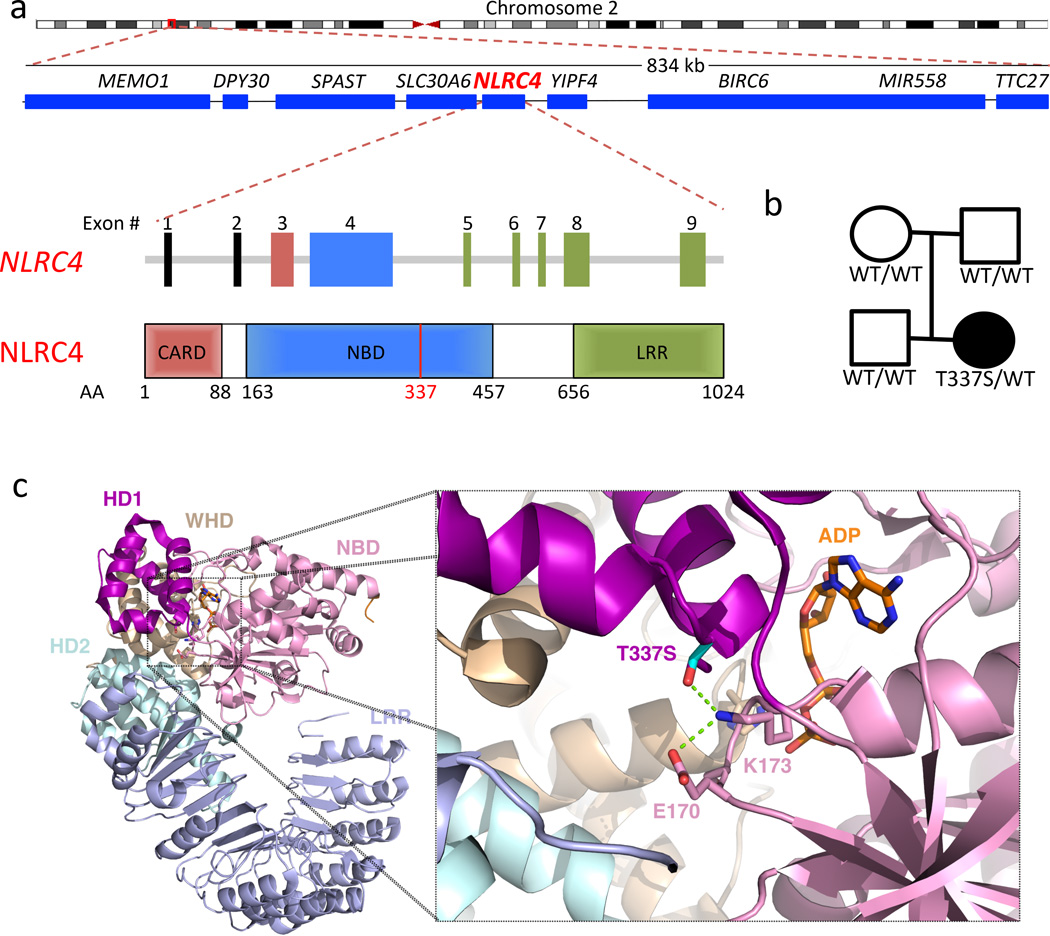
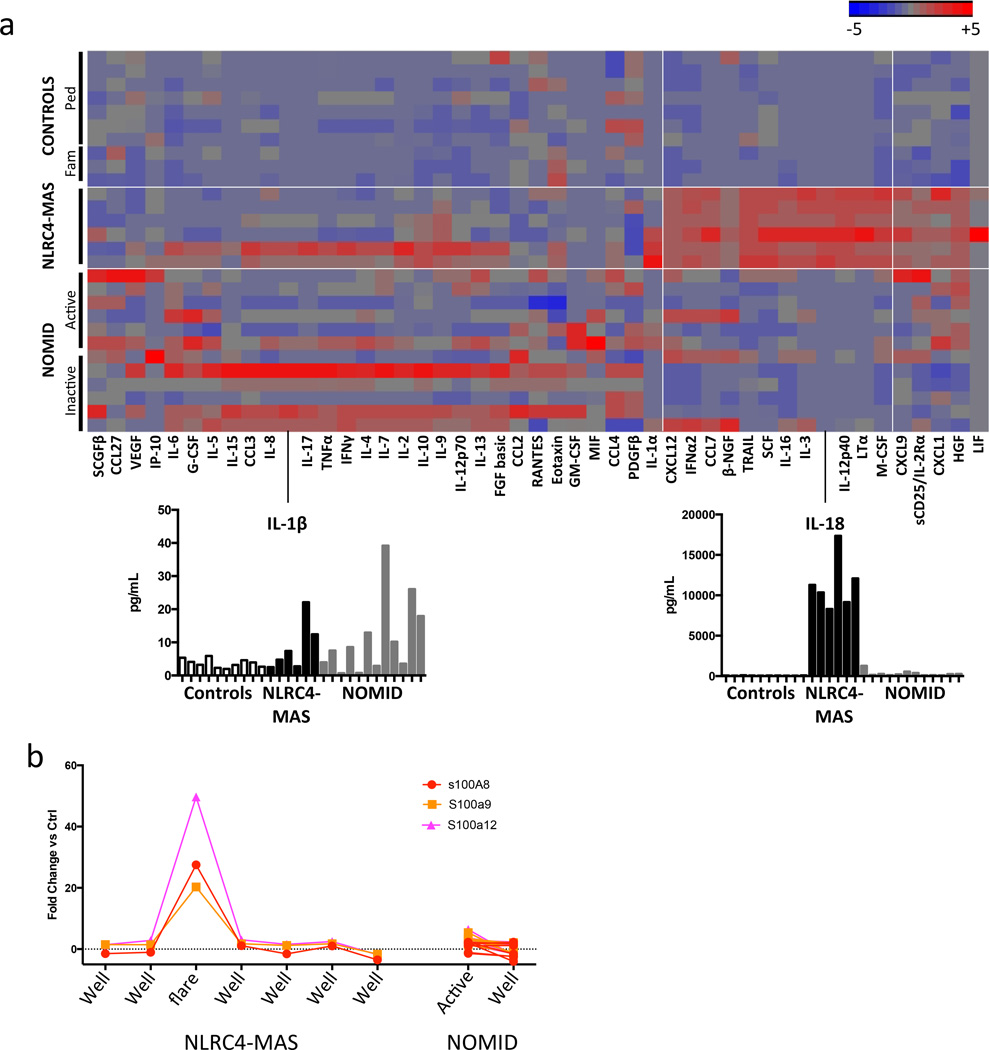
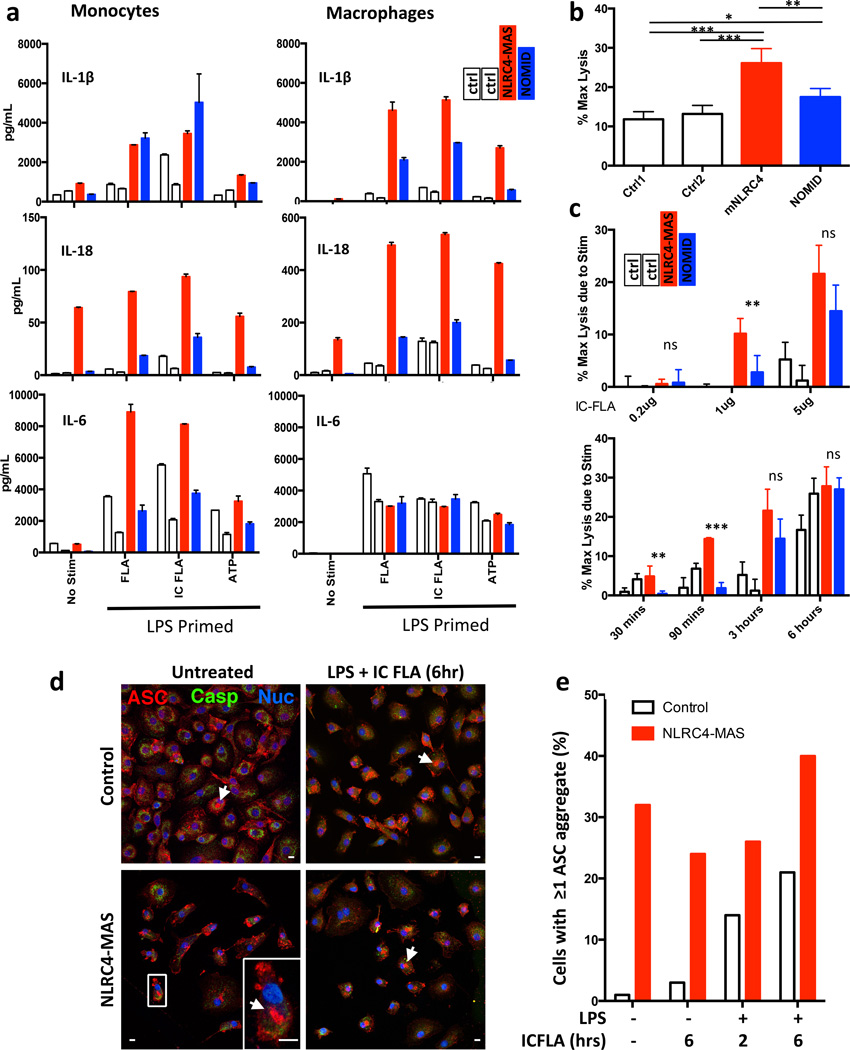
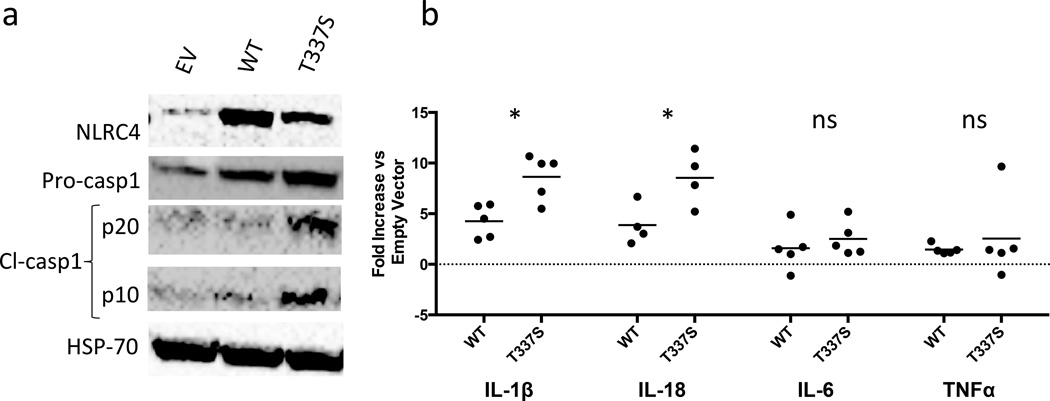
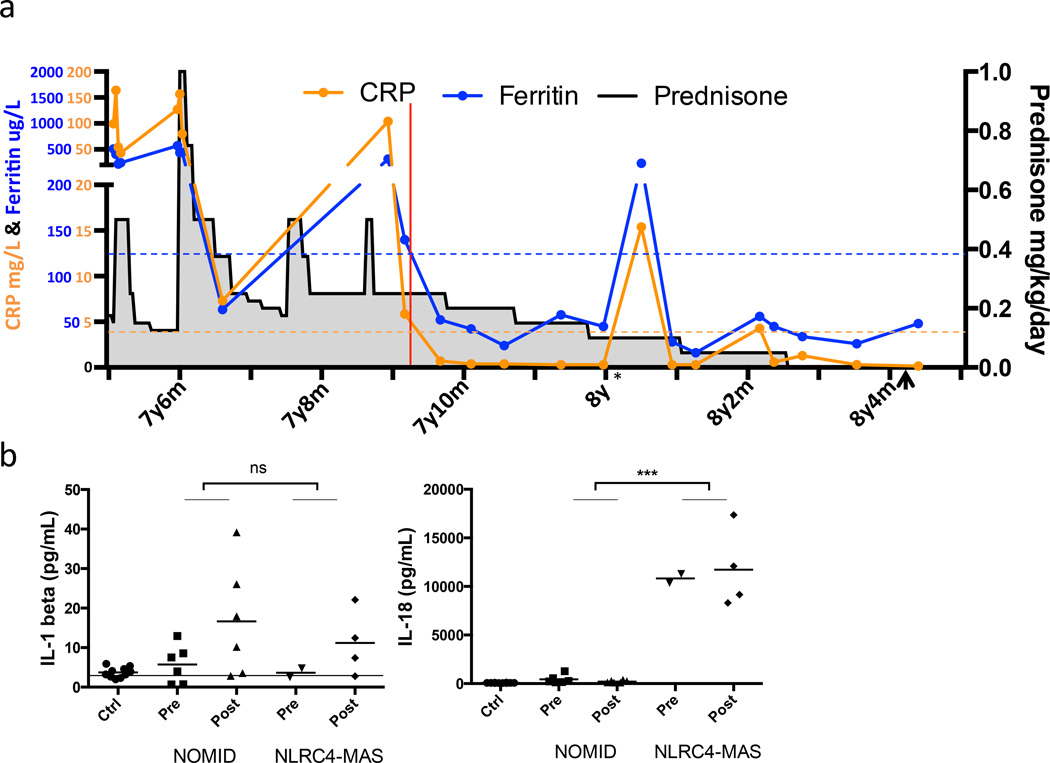
Inflammasomes are innate immune sensors that respond to pathogen- and damage-associated signals with caspase-1 activation, interleukin (IL)-1β and IL-18 secretion, and macrophage pyroptosis. The discovery that dominant gain-of-function mutations in NLRP3 cause the cryopyrin-associated periodic syndromes (CAPS) and trigger spontaneous inflammasome activation and IL-1β oversecretion led to successful treatment with IL-1-blocking agents. Herein we report a de novo missense mutation (c.1009A > T, encoding p.Thr337Ser) affecting the nucleotide-binding domain of the inflammasome component NLRC4 that causes early-onset recurrent fever flares and macrophage activation syndrome (MAS). Functional analyses demonstrated spontaneous inflammasome formation and production of the inflammasome-dependent cytokines IL-1β and IL-18, with the latter exceeding the levels seen in CAPS. The NLRC4 mutation caused constitutive caspase-1 cleavage in cells transduced with mutant NLRC4 and increased production of IL-18 in both patient-derived and mutant NLRC4-transduced macrophages. Thus, we describe a new monoallelic inflammasome defect that expands the monogenic autoinflammatory disease spectrum to include MAS and suggests new targets for therapy.
Figures
Comment in
-
NLRC4 gets out of control.Nat Genet. 2014 Oct;46(10):1048-9. doi: 10.1038/ng.3100. Nat Genet. 2014. PMID: 25257084
-
Autoinflammation: NLRC4 mutation causes rare autoinflammatory disease.Nat Rev Rheumatol. 2014 Nov;10(11):635. doi: 10.1038/nrrheum.2014.170. Epub 2014 Sep 30. Nat Rev Rheumatol. 2014. PMID: 25266450 No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
- Actions
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
