

Varying gestational age patterns in cesarean delivery: an international comparison
- PMID: 25217979
- PMCID: PMC4177602
- DOI: 10.1186/1471-2393-14-321
Varying gestational age patterns in cesarean delivery: an international comparison
Abstract
Background: While international variations in overall cesarean delivery rates are well documented, less information is available for clinical sub-groups. Cesarean data presented by subgroups can be used to evaluate uptake of cesarean reduction policies or to monitor delivery practices for high and low risk pregnancies based on new scientific evidence. We studied differences and patterns in cesarean delivery rates by multiplicity and gestational age in Europe and the United States.
Methods: This study used routine aggregate data from 17 European countries and the United States on the number of singleton and multiple live births with cesarean versus vaginal delivery by week of gestation in 2008. Overall and gestation-specific cesarean delivery rates were analyzed. We computed rate differences to compare mode of delivery (cesarean vs vaginal birth) between selected gestational age groups and studied associations between rates in these subgroups namely: very preterm (26-31 weeks GA), moderate preterm (32-36 weeks GA), near term (37-38 weeks GA), term (39-41 weeks GA) and post-term (42+ weeks GA) births, using Spearman's rank tests.
Results: High variations in cesarean rates for singletons and multiples were observed everywhere. Rates for singletons varied from 15% in The Netherlands and Slovenia, to over 30% in the US and Germany. In singletons, rates were highest for very preterm births and declined to a nadir at 40 weeks of gestation, ranging from 8.0% in Sweden and Norway, to 22.5% in the US. These patterns differed across countries; the average rate difference between very preterm and term births was 43 percentage points, but ranged from 14% to 61%. High variations in rate differences were also observed for near term versus term births. For multiples, rates declined by gestational age in some countries, whereas in others rates were similar across all weeks of gestation. Countries' overall cesarean rates were highly correlated with gestation-specific subgroup rates, except for very preterm births.
Conclusions: Gestational age patterns in cesarean delivery were heterogeneous across countries; these differences highlight areas where consensus on best practices is lacking and could be used in developing strategies to reduce cesareans.
Figures
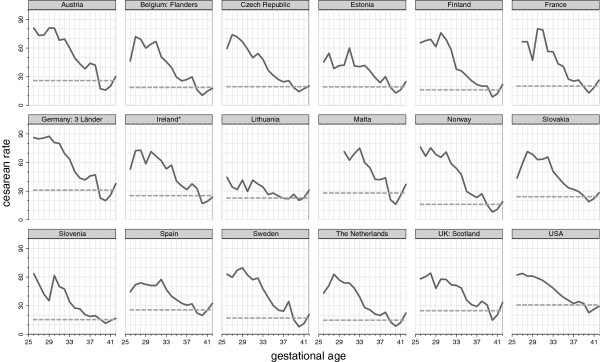
 cesarean rate by GA in completed weeks.
cesarean rate by GA in completed weeks.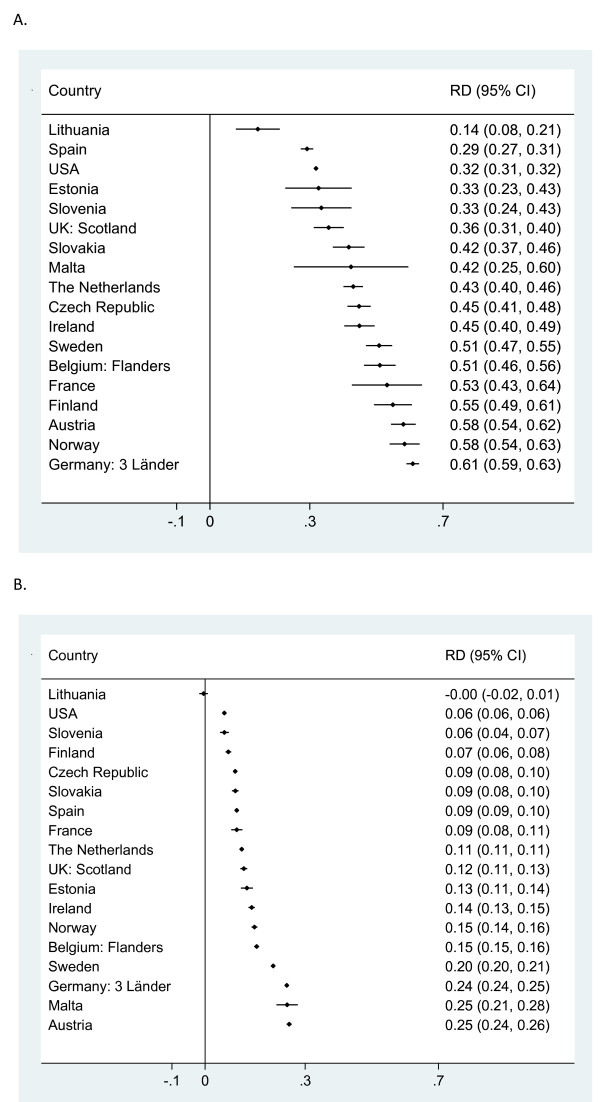
Similar articles
-
International variations in the gestational age distribution of births: an ecological study in 34 high-income countries.Eur J Public Health. 2018 Apr 1;28(2):303-309. doi: 10.1093/eurpub/ckx131. Eur J Public Health. 2018. PMID: 29020399 Free PMC article.
-
Maternal and newborn outcomes with elective induction of labor at term.Am J Obstet Gynecol. 2019 Mar;220(3):273.e1-273.e11. doi: 10.1016/j.ajog.2019.01.223. Epub 2019 Feb 17. Am J Obstet Gynecol. 2019. PMID: 30716284
-
Temporal Trends in Late Preterm and Early Term Birth Rates in 6 High-Income Countries in North America and Europe and Association With Clinician-Initiated Obstetric Interventions.JAMA. 2016 Jul 26;316(4):410-9. doi: 10.1001/jama.2016.9635. JAMA. 2016. PMID: 27458946 Free PMC article.
-
Cesarean section on request at 39 weeks: impact on shoulder dystocia, fetal trauma, neonatal encephalopathy, and intrauterine fetal demise.Semin Perinatol. 2006 Oct;30(5):276-87. doi: 10.1053/j.semperi.2006.07.009. Semin Perinatol. 2006. PMID: 17011400 Review.
-
The relationship between cesarean delivery and gestational age among US singleton births.Clin Perinatol. 2008 Jun;35(2):309-23, v-vi. doi: 10.1016/j.clp.2008.03.002. Clin Perinatol. 2008. PMID: 18456071 Review.
Cited by
-
What contributes to disparities in the preterm birth rate in European countries?Curr Opin Obstet Gynecol. 2015 Apr;27(2):133-42. doi: 10.1097/GCO.0000000000000156. Curr Opin Obstet Gynecol. 2015. PMID: 25692506 Free PMC article. Review.
-
Cesarean section and pregnancy outcomes of preterm premature rupture of membranes under different fertility policies in China.Transl Pediatr. 2021 Apr;10(4):973-983. doi: 10.21037/tp-21-144. Transl Pediatr. 2021. PMID: 34012845 Free PMC article.
-
International variations in the gestational age distribution of births: an ecological study in 34 high-income countries.Eur J Public Health. 2018 Apr 1;28(2):303-309. doi: 10.1093/eurpub/ckx131. Eur J Public Health. 2018. PMID: 29020399 Free PMC article.
-
Practical Experience of Establishing German Standard Level 1 Perinatal Center in Chongqing Health Care for Women and Children.Curr Med Sci. 2020 Oct;40(5):829-834. doi: 10.1007/s11596-020-2273-2. Epub 2020 Oct 29. Curr Med Sci. 2020. PMID: 33123898
-
Linking databases on perinatal health: a review of the literature and current practices in Europe.Eur J Public Health. 2016 Jun;26(3):422-30. doi: 10.1093/eurpub/ckv231. Epub 2016 Jan 10. Eur J Public Health. 2016. PMID: 26891058 Free PMC article.
References
-
- Euro-Peristat project with SCPE and Eurocat . European Perinatal Health Report: the health of pregnant women and babies in Europe in 2010. 2013.
-
- Villar J, Carroli G, Zavaleta N, Donner A, Wojdyla D, Faundes A, Velazco A, Bataglia V, Langer A, Narvaez A, Valladares E, Shah A, Campodonico L, Romero M, Reynoso S, de Padua KS, Giordano D, Kublickas M, Acosta A. Maternal and neonatal individual risks and benefits associated with caesarean delivery: multicentre prospective study. BMJ. 2007;335(7628):1025. doi: 10.1136/bmj.39363.706956.55. - DOI - PMC - PubMed
-
- Spong CY, Berghella V, Wenstrom KD, Mercer BM, Saade GR. Preventing the first cesarean delivery: summary of a joint Eunice Kennedy Shriver National Institute of Child Health and Human Development, Society for Maternal-Fetal Medicine, and American College of Obstetricians and Gynecologists Workshop. Obstet Gynecol. 2012;120(5):1181–1193. - PMC - PubMed
Pre-publication history
-
- The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2393/14/321/prepub
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
